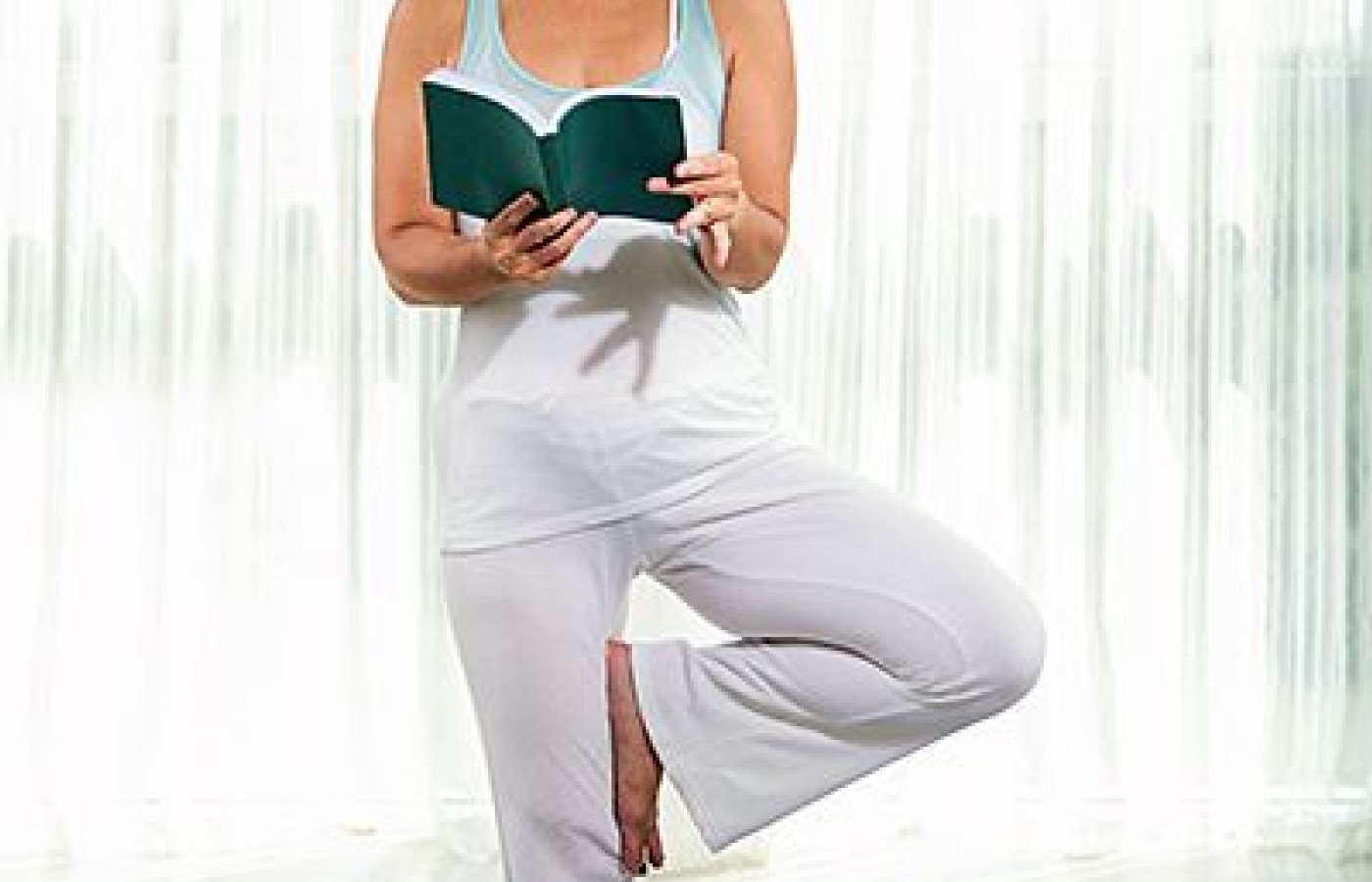
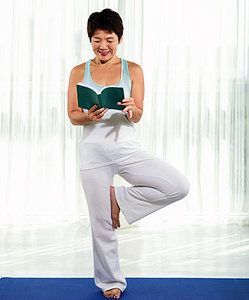
Essential Orthopedic Testing: Tests That Involve Standing on One Leg
K. Jeffrey Miller, DC, MBA
Since these tests have a common mechanism of performance (standing on one leg), there are differential diagnostic concerns during testing. The tests cannot be completely isolated from each other for performance. Standing on one leg alone without performing any of the additional maneuvers unique to the individual tests can cause a positive (pathological indicator) for more than one test.
In other words, just because the doctor believes they are performing the stork test it does not mean they will not see a positive response for Trendelenburg's test as well. Simply naming the test in the mind or in an examination procedure does not isolate the common mechanism of standing on one leg to a particular tissue and the presence or absence of pathology in that tissue.
When tests have common mechanisms of performance, applying the mechanism means that for the most part, all of the tests are being performed simultaneously. The only difference is which tissue / structure has pathology. The reaction of the pathological tissue, pain and/or dysfunction in a particular area is the indicator of which of the overlapping tests is positive.
This thinking is logical, but it is the reverse of how we teach orthopedic testing. Traditionally, we describe the name(s), the performance, the indicators of positive and negative findings, and then the pathology associated with a test.
Working from the mechanics of performance, standing on one leg stresses the patient's lower extremity, pelvis and lower back. The bones, ligaments, their joints, muscle and coordinating neurology of these structures are involved. It is difficult to isolate which tissue(s) is truly being tested other than through patterns of pain and dysfunction associated with a specific tissue.
In orthopedic testing, the doctor and/or patient should perform the maneuver(s) for the test, and the doctor should note the response and then select the pathology and name associated with that response. This is true for most orthopedic testing.
Dynamic Considerations
Focusing on performance here, there are a few dynamics that must be considered for their use. Balance is the first dynamic. Standing on one leg requires good balance. A patient without good balance may be a poor candidate for this series of tests. It is recommended that the patient be questioned about their balance and that simple coordination testing be performed prior to asking the patient to stand on one leg.
A second dynamic is lower extremity motor strength. A patient with weak lower extremities is also a poor candidate for one-legged testing. McNab recommends one-legged toe raises to evaluate calf strength in the lower extremities. Hoppenfeld recommends hopping on one foot to evaluate calf strength. Obviously if strength is a concern, these methods are no safer than the other one-legged tests.
Bilateral toe raises are safer and help determine if one-legged testing will be possible. Having the patient perform several repetitions will provide the necessary information to help determine safety for testing.
Lower extremity pathology is another dynamic. Pain and dysfunction from lower extremity pathology may interfere with or prevent standing on one leg. In these situations, if standing on one leg can be performed, it may be diagnostic for the lower extremity condition. Thessaly's test for meniscal pathology of the knee is an example.
Thessaly's is performed with the patient standing on one leg. This brings additional differential diagnostic issues into play. Pathology associated with the knee and ankle can be identified through standing on one leg. These structures cannot be considered as isolated just because the examiner is focused on the lower back and pelvic region.
The dynamics described above obviously make performing any of these tests more difficult than performing other types of tests. One item that can help remove some of the challenges is a handrail. Installing a vertical handrail, like those typically seen in baths and showers, on the examination room wall can help. The patient can stand next to the rail and hold onto it during testing to maintain balance. Vertical orientation of the handrail works better than horizontal orientation to allow for varying patient heights.
Once the patient's balance and strength have been assessed, brief testing on one leg can begin. Table 1 describes the test names, performances, interpretations and associated pathologies for lower back and pelvic region tests performed while standing on one leg. All tests should be performed bilaterally unless pain / dysfunction initially prevents continuation of testing.
Table 1: Tests Involving Standing onOne Leg – Subtle Differences and Interpretations
Test Name
Performance
Positive-Pathological Indications
Pathology
Trendelenburg's
Standing on one leg
Drooping of the pelvis on the contralateral side ofthe weight-bearing leg
Weakness or tear of the gluteus medius muscle; hipjoint pathology
One-Legged-Standing Lumbar Extension
Standing on one leg with extension of the lumbarspine
Pain in the lower back (unilateral / bilateral)
Pars interarticularis fracture (unilateral pain);lumbar instability (bilateral pain); facet pain
McBride's
Standing on one leg while drawing the contralateralleg to the chest
Relief of lumbar spine pain
Facet pathology
Gillet's (Stork)
Patient stands while examiner palpates the S2 spinousprocess and the PSIS on one side. Patient raises the leg on the side the examineris palpating so the examiner can assess motion in the SI joint. The PSISshould move posterior to inferior.
Pain in the hip (coxa) joint, SI joint or lumbarspine
Unspecified pathology in the area of pain
*Replicates Hoppenfeld's test for strength testing ofcalf musculature
Differential Diagnosis
During testing, just the action of standing on one leg can irritate several structures if they are pathological. The most obvious is weakness of the gluteus medius muscle, since standing on one leg is the only movement used for Trendelenburg's test and no additional movements are required.
The testing position causes an increase in the lumbar lordosis and increases the weight-bearing load on the facet joints, SI and hip joints on the weight-bearing side. This could irritate a variety of pathologies in these joints.
If the pars interarticularis is fractured, it could hurt even without the additional extension of the lumbar spine used in the one-legged standing test or the hop associated with the hopping test.
Bringing the non-weight-bearing leg to the chest exaggerates the motion used in Gillet's test. If the examiner palpates the landmarks for the test and has the patient bring the non-weight-bearing leg to the chest, Gillet's and McBride's tests are performed together. The examiner can feel and observe the motion of the SI joint (Gillet's) and inquire about changes in lumbar region pain (McBride's). This method also allows better stabilization of the patient, as the examiner is in contact with the patient.
For practical use, if the examiner palpates the contacts necessary for performing Gillet's test and asks the patient to perform McBride's test, the drooping of the pelvis in Trendelenburg's test could also be seen. The motion of the pelvis for Gillet's test can be assessed. Decreased lumbar pain particular to McBride's can be identified. Increases in lumbar, SI or hip pain assessed by one-leg standing and hopping can also be identified.
If none of the signs significant to the tests in this group is present, it is reasonable to consider all of the tests to be negative. If signs significant to a test or tests in this group are present, the examiner must consider the differences in positive responses among the tests and should perform the tests individually.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.