Blaming the Gluteus Medius, Overlooking the Deltoid
Justin Hildebrand, DC
The gluteus medius (Gmed) is commonly written about, strengthened and blamed for many conditions, and rightfully so. After all, the Gmed plays a role in pelvic stability, hip motor control and lower-quarter dynamic movements. This muscle stabilizes the pelvis and lumbar spine, and can move the hip in abduction, internal rotation, external rotation, extension and even flexion. The deltoid, on the other hand, is hardly written about and never really blamed for conditions – although it absolutely should be.
Deltoid Biomechanics and Patterns of Dysfunction
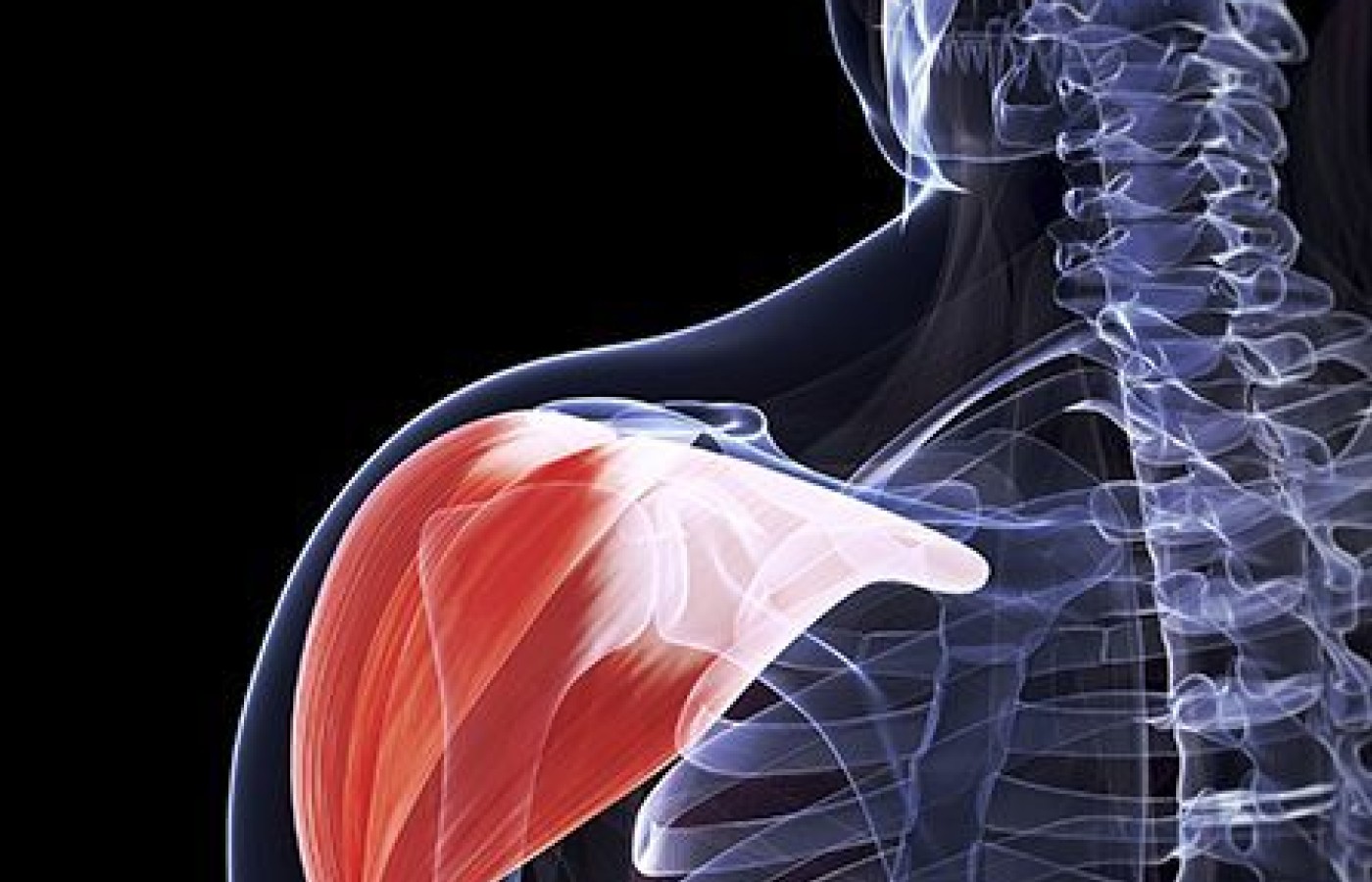
Functionally, the deltoid can be divided into three sections: anterior, lateral (middle) and posterior. The anterior deltoid abducts, flexes, internally rotates and horizontally adducts the humerus. The middle deltoid abducts and slightly flexes the arm and posterior deltoid. Much like the posterior fibers of the Gmed play a significant role in hip motion, the deltoid plays a role in almost all shoulder motions, including movements involving the AC joint, GH joint and scapulothoracic joint.
Neumann1 describes the posterior deltoid as a humeral adductor in anatomical position, an external rotator in the horizontal plane, and a humeral extensor in the sagittal plane. Therefore, a lack of abduction could contribute to a weak anterior and middle deltoid, and/or a tight or facilitated posterior deltoid. Oscar2 adds that the posterior fibers, when becoming the prime movers of external rotation, create anterior humeral glide, decentrating the glenohumeral joint and limiting posterior glide.
Oscar also describes that the middle or lateral deltoid can become overactive or dominate with associated supraspinatus inhibition. This dysfunction can lead to increased superior glide of the humerus and contribute to glenohumeral impingement syndrome. GH impingement leads to supraspinatus injury and the cycle of reciprocal inhibition continues. The anterior deltoid can pull the shoulder into a rounded position, contributing to rounded shoulders and creating an imbalance of the shoulder external rotators and posterior capsule.2
During performance of the shoulder abduction functional screen, an overactive levator scapulae and/or upper trapezius can cause superior movement of the shoulder girdle. Ipsilateral cervical lateral flexion represents a failure of this screen and also suggests overactivity of the levator and upper trap. This repetitive motion can inhibit and decrease the activity of the deltoid.
In chronic shoulder abduction dysfunction, postural findings of deltoid inhibitions can be observed. Page states that the deltoid is atrophied in patients presenting with impingement and exhibits lower levels of EMG activation.3 Lack of deltoid tone presents as oblique flattening in the anterior lateral shoulder.
Rehabbing the Dysfunctional Deltoid: Exercise Options
From a rehabilitation standpoint, the dysfunctional deltoid responds clinically with small, simplistic exercises. Large movements and lever arms increase the activity of the tonic musculature and feed the patient's dysfunction. Bent-elbow isometric shoulder abduction at 0-15 degrees and side-lying 5-15-degree arm raises can activate the deltoid and supraspinatus, while limiting the overactivity of the levator and trap. Standing shoulder extension self-mobilizations focusing on not rolling the humeral head forward or gliding superior can help stretch the anterior deltoid and AC joint, while activating the posterior fibers. Deltoid retraining may prove to be as vital as Gmed exercises in rehabilitation.
References
Neumann DA. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. St. Louis, MO: Mosby Elsevier, 2010.
Oscar E. Corrective Exercise Solutions to Common Hip and Shoulder Dysfunctions. Santa Cruz, CA: On Target Publications, 2012.
Page P. Shoulder muscle imbalance and subacromial impingement syndrome in overhead athletes. Int J Sports Phys Ther, March 2011;6(1):51.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.