It is well-known that metabolic changes in children, including insulin resistance, may be responsible for accelerated biological maturation, manifested as accelerated bone age. This may lead to hypertension and cardiovascular disease in the future. A recent study reports that advanced skeletal maturation should be considered an independent marker for the development of primary hypertension (PH) in children.1
This was a cross-sectional control study of children diagnosed with PH vs. normotensive control subjects to examine the prevalence of advanced bone age (BA) and its role in predicting PH in children and adolescents. The study utilized dual X-ray absoptiometry-derived hand scans of 54 newly diagnosed children and adolescents with PH and 54 healthy controls matched for body mass index, age and sex. Chronological age (CA), body height, body weight, BMI and blood pressure were assessed. Results were as follows:
Ossification Centers and Epiphyseal Growth-Plate Maturation of the Carpals, Including the DIPS and PIPs*
Fig. 1: The Risser sign uses the appearance of the iliac apophysis to assess bone age. The apophysis appears laterally along the iliac crest and moves toward the spine with the approach of skeletal maturation.
I am not suggesting that all your pediatric patients need to have their BA assessed. However, if X-rays have been taken, consider looking for signs of accelerated BA, especially in overweight patients. Disorders that bring the pediatric patient into chiropractic offices are back pain or scoliosis. An AP lumbar film is often taken, depending on the history and symptoms. If an AP lumbar film is available no further X-rays are needed. Just use the Risser's sign to determine if accelerated BA is present. Further evaluation can then be performed to confirm the presence of accelerated BA.
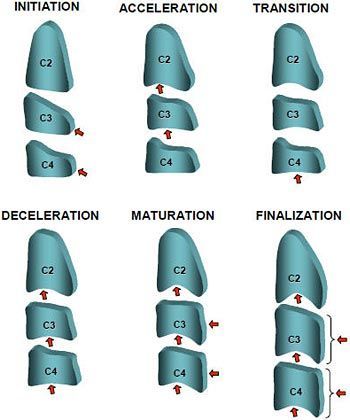
One can also use a lateral cervical spine X-ray to determine growth and maturation using Lamparski's method.3 This method often assesses the morphological changes associated with growth and maturation of the cervical vertebrae in six stages; also very legitimate. Kamal, et al., reported a comparative study evaluating the hand/wrist and cervical vertebrae and demonstrating that cervical vertebrae can be used with the same confidence as hand/wrist radiographs to evaluate skeletal maturity.4
The Risser Sign: Grade and Average Age (Boys/Girls)
Fig. 2: Comparison of the Risser sign and maturation of the hand/wrist.
The Risser sign uses the appearance of the iliac apophysis to assess BA. The apophysis appears laterally along the iliac crest and moves toward the spine with the approach of skeletal maturation. Using the Risser's sign, one can measure the growth left in the spine. This method is generally used to help to determine the potential for progression of scoliosis, but can certainly be used for determining BA. Grading (based on iliac crest divided into four quadrants) involves the following:
Risser 1: 25 percent iliac apophysis ossification; anterior superior iliac spine (anterolateral). Seen in pre-puberty or early puberty.
Risser 2: 50 percent iliac apophysis ossification. Ossification extends halfway across iliac wing. Seen immediately before or during growth spurt.
Lamparski's method established a maturational pattern for cervical vertebrae using vertebrae C2-C6, consisting of six stages.3 This method of evaluating skeletal maturation is now called the cervical vertebrae maturation indicators (CVMIs) and are as follows: initiation (stage I); development of concavities on the lower borders of the vertebral bodies (stage II); increase of the anterior portion and of the total height of these vertical bodies causing changes in their shape (stage III); changing from a wedge shape to a rectangular shape (stage IV), and later, to a square (stage V); and finally, presenting a predominance of height over width (stage VI).
The vertebral maturity indicators are the same for males and females. The CVMI is considered to have the same clinical value as the hand-wrist evaluations. As in most maturation evaluations, each stage of vertebral development occurs earlier in females than in males.
Because of the rise in chronic diseases in children, we need to be more acutely aware of the signs associated with early onset of chronic disease. Accelerated bone maturation is one sign. Parents should be aware that skeletal and pubertal maturation is accelerated with obesity. Most researchers believe that skeletal maturation cannot be reversed, but nutrition and weight loss can slow the acceleration.
Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development of the Hand and Wrist, 2nd Edition. Stanford, Calif.: Stanford University Press, 1959.
Lamparski DG. "Skeletal Age Assessment Utilizing Cervical Vertebrae." Master's thesis, University of Pittsburgh, 1972.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.