There is vast literature about the accessory bones in the skeleton: some will certainly defy radiologic detection because of the limitations of radiographic projections of the wrist. A large number however are detectable. The main reason for mentioning the existence of the accessory bone is to distinguish it from a recent trauma. Several accessory bones are not congenital, but acquired ossifications of post-traumatic degenerative etiology. In fact the os centrale carpi and the os triangulare are only ossicles that are considered definitely congenital.1
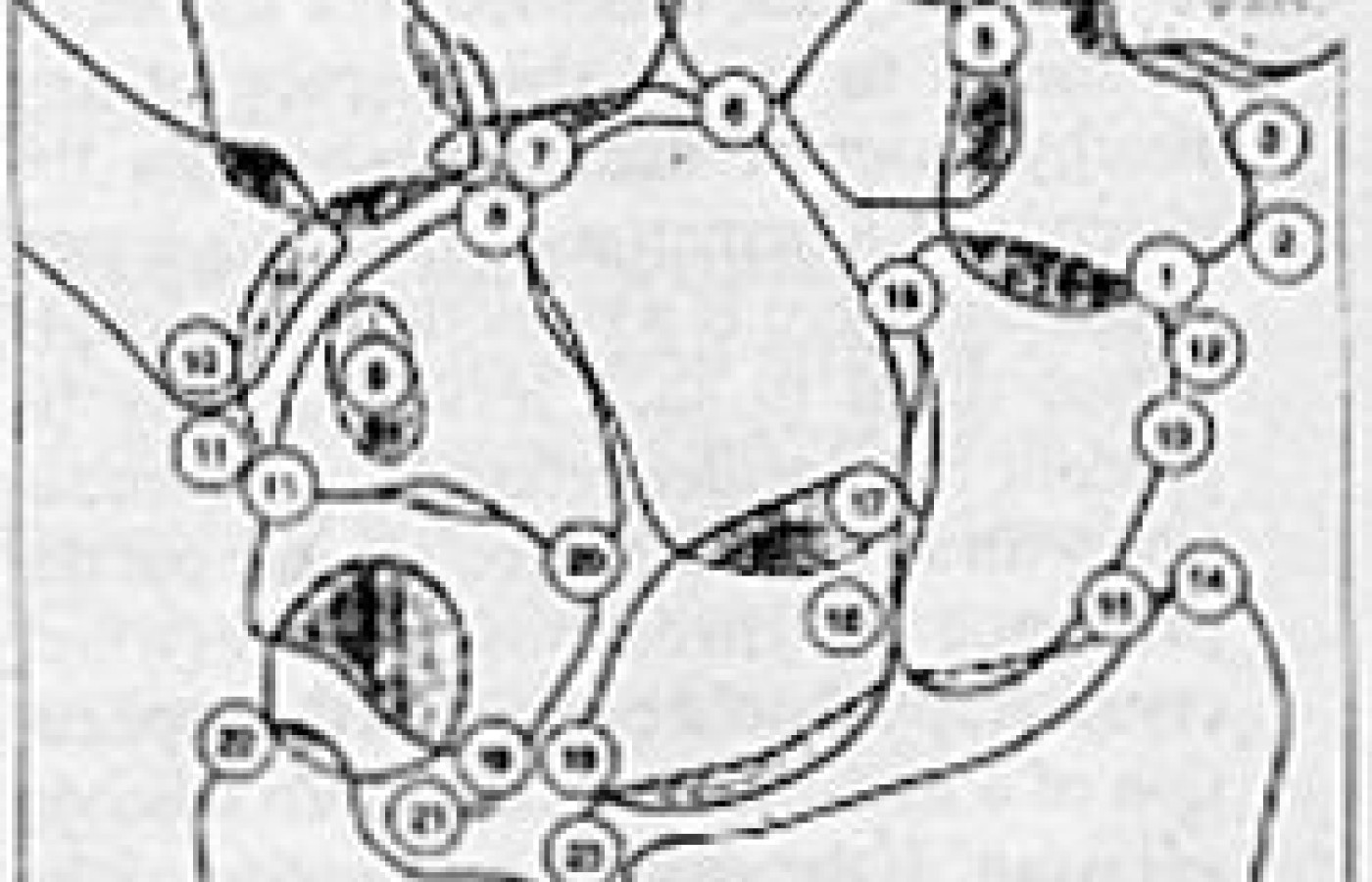
Key to Figure 1:
epitrapezium
calcification (bursa or flexor carpi radialis)
paratrapezium
secondary trapezium
secondary trapezoid
os styloideum
Gruber ossicle
secondary capitate
os hamuli proprium
os versalianum
os ulare externum (bursal or tendinous calcifications)
os radiale esternum
traumatic avulsions
unfused ossification center of the radial styloid process
intercalary ossicle between scaphoid and radius (os paranaviculare)
os centrale carpi
hypolunate
epilunate
accessory ossicle between lunate and triquetrum
epipyramis
triangulare
unfused ossification center of the ulnar styloid process
small ossicle at the radioulnar articulation
Figure 1 demonstrates the potentially visible accessory bones that can be present on a PA view of the wrist. Many ossicles probably correspond to a capsular ossification as a manifestation of degenerative changes rather than a true anomaly. The epitrapezium may represent bursal calcification or tendon calcification. The hook of the hamate ossifies independently and if it does not fuse, it remains isolated and is seen as an accessory bone, the os hamuli proprium. When seen in the lateral view it can be mistaken for a fracture. The os ulnare externum can be an acquired ossification or calcification and should be considered in the differential diagnosis. A separate ossification center can occur at the radial styloid process persisting to imitate a super numerary skeletal element. Along the ulnar aspect of the styloid process, a small ossicle is occasionally found. Between the scaphoid and the articulating surface of the radial styloid process. This may also be ossification in the tendon or tendon sheath.
The most important factor is to determine if the ossicle is due to recent trauma or if it represents an old degenerative change or an anomaly. If there is a question as to the most accurate diagnosis, take an x-ray of the opposite wrist. With an anomaly frequently they are bilateral. If there is still a question, repeat the study in 14 to 21 days. If it is a recent injury there should be evidence of healing present on the later study indicating the accessory element was a recent injury.
Reference
1. Kohler and Zimmer: Borderlands of Normal and Early Pathologic Findings in Skeletal Radiology. Thieme, 1993.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.