Now that we are in the holiday season and people are just getting back to winter sports, I'd like to review a common injury - one I personally would like to avoid!
The anterior cruciate ligament is the most commonly injured ligament in the knee. A tear in this ligament usually occurs following a sudden valgus impact, and is generally caused by a sudden twisting motion, as in the feet being planted in one direction with the knees turned in the opposite direction. (The posterior cruciate ligament is generally injured in direct impact.)
Knees that are unstable as a result of anterior cruciate ligament tears put patients at risk for early degenerative joint disease and subsequent damage to other structures of the knee.
There are several orthopedic tests for evaluating an anterior cruciate injury, but the Lachman's test is touted as the most specific and reliable. (I must confess that I do at times have trouble with orthopedic tests. I like to see what's going on!)
Injury to a cruciate ligament may not cause pain. Rather, the person may hear a popping sound, and the leg may buckle. An MRI is very accurate in detecting a complete tear, but arthroscopy may be the only reliable means of detecting a partial tear. (MRI is 97% accurate compared to arthroscopy in diagnosing ACL tears)
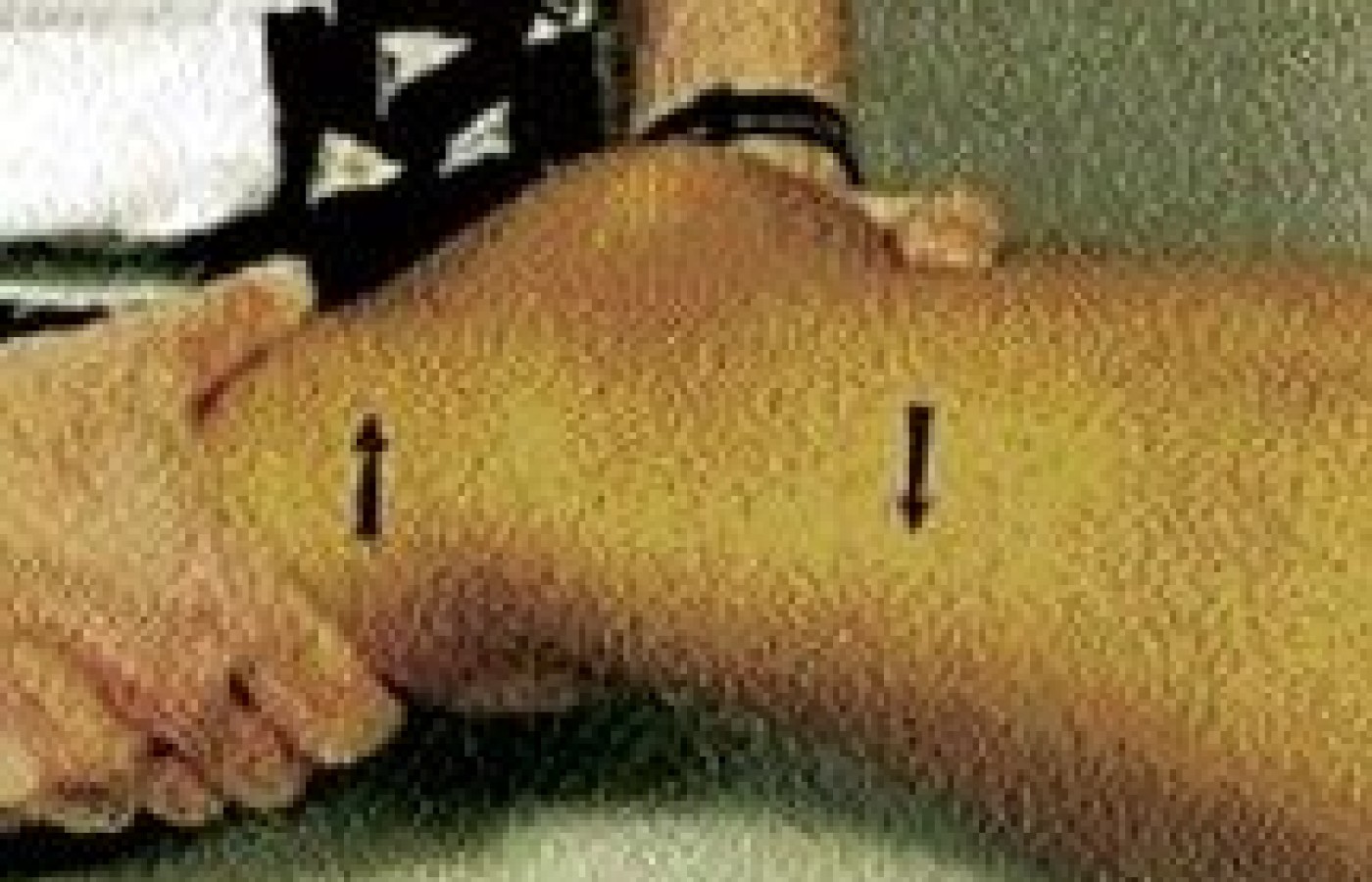
Figure 1: Lachman's test of the right knee. The examiner uses the right hand to place anterior force on the lower leg while simultaneously using the left hand to place posterior force on the distal thigh. A good end point should be felt. Hands are reversed to test the left knee.
For an incomplete tear, the patient may respond to conservative treatment, including an exercise program to strengthen surrounding muscles. A protective knee brace may also help during activity. For a completely torn anterior cruciate ligament in an active athlete, surgery is generally recommended. The surgeon may reattach the torn ends of the ligament or reconstruct the torn ligament by using a graft ligament from the patient (autograft) or from a cadaver (allograft). Although repair using synthetic ligaments has been tried, the procedure has not yielded results as good as those using human tissue. One of the most important elements in a patient's successful recovery after cruciate ligament surgery is following an exercise and rehabilitation program for four to six months. Successful surgery and rehabilitation will allow the patient to return to a normal lifestyle.
Figure 2: Example of anterior cruciate tear in young patient.
References
Andrews M, Noyes F, et al. Anterior cruciate ligament allograft reconstruction in the skeletally immature athlete. Am J Sports Med, Vol. 22, No.1, pp. 48-54, 1994.
Bertin K, et al. Ligament injuries associated with physeal fractures about the knee. CORR, No. 177, pp. 188-195, July/ August 1983.
Clanton T, DeLee J, et al. Knee ligament injuries in children. JBJS, 61-A, No. 8, pp. 1195-1201, December 1979.
DeLee J, et al. Anterior cruciate ligament insufficiency in children. CORR, No. 172, pp. 112-8, Jan/Feb 1983.
Engebretsen L, et al. Poor results of anterior cruciate ligament repair in adolescence. Acta Orthop Scand 1988; 59(6): pp. 684-6.
Kannus P, et al. Knee ligament injuries in children. JBJS, 70-B, No. 5, pp. 772-6, November 1988. Lipscomb B, Anderson A, et al. Tears of the anterior cruciate ligament in adolescents. JBJS, 68-A, No. 1. pp. 19-28, Jan 1986.
McCarroll J, Shelbourne K, et al. Anterior cruciate ligament injuries in the young athlete with open physes. Am J Sports Med, Vol. 16, No. 1, pp. 44-47, 1988.
Parker A, Drez D, et al. Anterior cruciate ligament injuries in patients with open physes. Am J Sports Med, Vol. 22, No. 1, pp. 44-47, 1994.
Polly D, et al. The accuracy of selective MRI compared with the findings of arthroscopy of the knee. JBJS, 70-A, No. 2, pp. 192-8, Feb 1988.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.