Editor's Note: This is the second is a series of "Dynamic Diagnosis" shorts by Dr. Miller as part of his Continuing Your Education column.
When it comes to conditions that are responsive to chiropractic care, facet syndromes are a perfect example. They are easy to diagnose and manipulation has a high rate of effectiveness in their treatment.
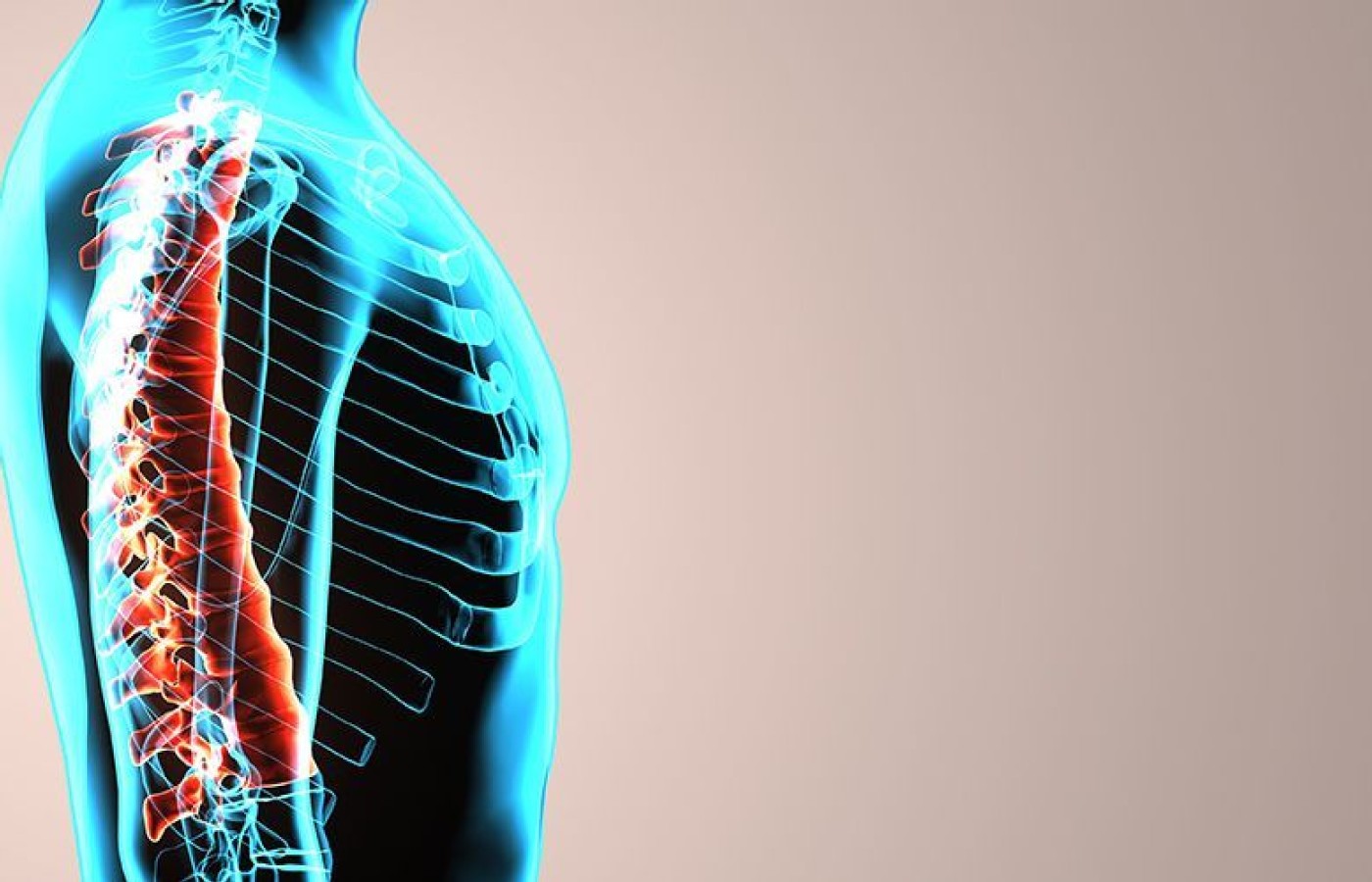
The facet joints are similar to and slightly smaller than the interphalangeal joints of the fingers and toes. They bear weight, allow and restrict movements of the spine, and contribute to spinal stability. Let's take a quick look at facet-joint pathology, how to identify it and appropriate treatment options.
Common Sources of Pathology
Facet joints are subject to pathology from several sources. Facet joint capsules become impinged between the articular surfaces of the joint, resulting in fixation – AKA segmental dysfunction (the classic facet syndromes).
Hyperflexion and hyperextension injure facet joints. Loss of disc height results in overlapping of the facet articular processes (imbrication). Arthritic changes or arthrosis develops in facet joints secondary to trauma or disc degeneration. Synovial cysts are common in facet joint capsules. Fracture of facet articular processes can occur.
While synovial cysts and fractures are not treatable through chiropractic methods, the other pathologies are and respond well.
Differential Diagnosis
Pain from facet joints is usually a diffuse, sclerotome-like pain in the associated spinal region. Pain can also refer to distant sites. In the cervical spine, the arms and mid-thoracic spine are affected. In the lumbar spine, the legs are affected.
Inexperienced clinicians often confuse the referred symptoms with radiculopathies. The differential diagnosis is easy. Facet syndromes do not result in positive nerve root tension signs, while radiculopathies do.
Diagnostic Testing, Key Findings and Clinical Care
A patient presenting with a facet syndrome can display one or more clinical findings, including antalgic posturing: the patient leans away from the affected side. For example, if a left facet is painful, the patient leans to the right. If the facets on both sides are painful, the patient flexes forward.
Extension is also more painful than flexion in facet syndromes. Avoidance movements, in which the patient avoids placing strain on the facet joints, are frequent. An example is flexion of the knees when moving from lumbopelvic flexion to lumbopelvic extension. Another example is the nose and chin deviating from the midline when the patient moves from cervical flexion to cervical extension.
Orthopedic tests that result in facet extension and/or rotation can cause facet pain. In the cervical spine, the maximum foraminal compression and sphinx tests are good examples. Sphinx test also applies to the thoracic and lumbar regions. Additional tests for the lumbar region are Milgram's and Kemp's.
Facet syndromes are not viewed to be as severe as disc disorders. However, facet syndromes are still a significant pathology and have substantial effects on a patient's health, function and activities of daily living. Manipulation is the primary mode of care. Rest, ice, interferential current and stretching are also helpful.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.