After 7 million years of adapting to upright postures, the lumbar spine and pelvis have become remarkably adept at managing ground-reactive forces associated with running. In fact, the intervertebral discs are so strong when standing upright that it is almost impossible to herniate a disc while walking or running: even the sudden application of extreme vertical forces will cause the vertebral endplates to fracture before the intervertebral discs herniate.
Nonetheless, gait cycle-related low back injuries do occur, and they can usually be related to a variety of biomechanical problems, ranging from muscle imbalances to limb-length discrepancy.
Biceps Femoris Tightness
According to Vleeming, et al.,1 an overlooked biomechanical cause of low back pain is tightness in the biceps femoris muscle that increases tension in the sacrotuberous ligament, effectively blocking the range of sacral nutation necessary for shock absorption.
Treatment in this situation involves identifying the various factors responsible for maintaining biceps femoris muscle tension and taking corrective action (e.g., biceps femoris muscle tightness may result from joint dysfunction in the lower lumbar spine and/or quadriceps / hamstring muscle imbalances).
Chiropractic adjustments are often necessary to restore motion to the damaged joints, and specific stretches / exercises should be prescribed to lengthen and strengthen the hamstrings, piriformis, multifidus, and erector spinae.
Weakness of the hip abductor musculature is perhaps the most common cause of low back pain in runners. Because the gluteus medius and minimus function to keep the pelvis in a nearly horizontal position during stance phase, weakness of these muscles will cause the pelvis to tilt in the frontal plane, allowing the lumbar spine to laterally flex excessively.
The exaggerated lumbar lateral flexion may result in chronic injury to the lower lumbar spine, especially if the core muscles are weak. Core weakness is also problematic when the hip flexors are excessively tight because the lumbar spine is allowed to hyperextend during propulsion.
Treatment
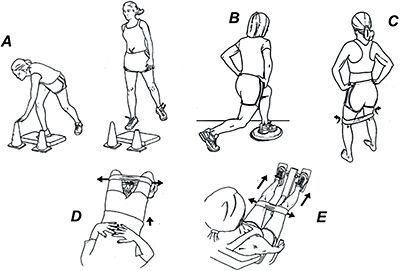
Effective treatment requires strengthening the abdominal musculature and improving flexibility in the hip flexors. This can be accomplished with exercises (see figure) that target the hip extensor and abductor musculature. These exercises are particularly effective when performed on unstable surfaces, such as a balance pad; and to enhance neural drive, the exercises can be performed by holding each position for up to 60 seconds.
HIP ABDUCTOR EXERCISES A) Single-leg cone touch on unstable surface. B) Balance disk lunge. C) Standing band piriformis exercise. D) Bridge while isometrically tensing hip abductors. E) Leg press with band around knees, producing a co-contraction between gluteus maximus and gluteus medius.
In addition, it is often necessary to perform gait retraining in which the athlete runs on a treadmill in front of a mirror and consciously minimizes frontal-plane motion of the pelvis.
Structural Limb-Length Discrepancy
Another somewhat controversial cause of gait-related low back pain is structural limb-length discrepancy. Although several studies suggest limb-length differences are not associated with pain,2-3 the majority of research confirms a clinical connection between low back pain and limb-length discrepancy.
By comparing the prevalence of limb-length discrepancies between 653 low back pain patients and 359 controls (the discrepancies were confirmed with radiographs), Friberg4 found that individuals with LBP were 1.7 times more likely to present with discrepancies greater than 5 mm, and 5.3 times more likely to have discrepancies greater than 15 mm.
This is consistent with a review of the literature by Giles and Taylor,5 who combined data from five separate studies to evaluate a total population of 1,806 subjects in which limb lengths were measured with radiographs.
In four of five studies, 13-22 percent of the population that sought medical attention for low back pain had a discrepancy of 10 mm or more, compared to 7 percent with no history of low back pain. This is consistent with their own radiographic study of 217 people in which 18.3 percent of the population with low back pain had a limb-length discrepancy greater than 10 mm, compared to only 8 percent of subjects with no complaints of low back pain.
Treatment
Structural limb-length discrepancies can be effectively treated with the appropriately sized lift. In the study by Giles and Taylor, subjects treated with shoe lifts reported significant reductions in pain and lost days from work, along with increases in their overall range of motion when evaluated at four-month follow-up.5
While the majority of literature supports the connection between low back pain and structural limb-length discrepancies, the connection between functional discrepancies and low back pain is more controversial.
While functional limb-length discrepancy can occur when hypertonicity in the suprapelvic and/or pelvic musculature produces a pelvic torsion when measured in an unloaded condition, this type of limb-length discrepancy can be readily treated with myofascial release and specific home stretches. Quadratus lumborum stretches are especially helpful in managing functional limb-length discrepancies.
The Role of Manipulation
In contrast, a common misconception among chiropractors, physical therapists and massage therapists is that the ilium can subluxate on the sacrum and lock in that position to produce a functional limb-length discrepancy capable of producing chronic low back pain. Despite the widespread belief that the sacroiliac joint can subluxate, there is little evidence to support this.
In fact, the notion that the ilium or sacrum can subluxate and be repositioned with manipulation was refuted in a roentgen stereophotogrammetric analysis (RSA) study by Tullberg, et al.6 After embedding tantalum beads in the sacrum and ilium of 10 patients with sacroiliac joint dysfunction, these authors evaluated the position of these bones before and after high-velocity manipulation of the sacroiliac joint.
Using advanced RSA testing, Tullberg, et al., conclusively demonstrated that manipulation and subsequent muscle-energy mobilization had no effect on the location of the sacrum or ilium in any of the subjects tested.
Because the accuracy of RSA testing identifies bony shifts as small as 0.2 mm, the authors state that twisting of the pelvis could not be the result of shifting of the sacrum or ilium, and that future studies should evaluate the effects of sacroiliac manipulation on the neighboring soft tissues and not on skeletal positioning.
The research by Tullberg, et al., makes it clear that manipulation does not reposition a vertebra from a misaligned position to an aligned position. Rather, it is likely the clinical success associated with manipulation can be related to the fact that manipulation breaks up adhesions present in the zygopophyseal joints of the spine,7 improves movement asymmetries8-9 and/or stimulates mechanoreceptors – thereby reducing spinal muscle excitability, enhancing proprioception and reducing pain.10
While manipulation has been proven effective for the management of acute low back pain,11-12 a prospective placebo-controlled study by Senna and Machaly13 demonstrates that long-term chronic low back pain sufferers respond best to maintenance manipulations performed bimonthly for up to nine months. The authors suggest the occasional manipulations may allow for the "early treatment of any emerging problem, thus preventing future episodes of low back pain."
Given the massive economic burden ineffective treatment protocols place on our already stressed health care system, proven treatment regimens incorporating a range of readily available and relatively inexpensive conservative interventions such as orthotics, lifts, rehabilitative exercises, and manual therapy have been shown to provide effective, long-term solutions for the majority of running-related injuries.
References
Vleeming A, Snijders C, Stoeckart R, Mens J. The Role of the Sacroiliac Joint in Coupling Between Spine, Pelvis, Legs and Arms. In: Vleeming A, Mooney V, Dorman T, et al. (eds). Movement, Stability and Low Back Pain: The Essential Role of the Pelvis. New York: Churchill Livingstone 1999: pp. 91-102.
Broadhurst N, Bond M. Pain provocation for the assessment of sacroiliac joint dysfunction. J Spinal Disorders, 1998;11:341.
Hellsing A. Leg length inequality. A prospective study of young men during their military service. Up J Med Sci, 1988;93:245–53.
Friberg O. Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality. Spine, 1983;8:643-51.
Giles LGF, Taylor JR. Low-back pain associated with leg length inequality. Spine, 1981;6:510-21.
Tullberg T, Blomberg S, Branth B, et al. Manipulation does not alter the position of the sacroiliac joint: a roentgenstereophotogrammetric analysis. Spine, 1998;23:1124-1128.
Cramer G, Tuck N, Knudsen J, et al. Effects of side-posture positioning anti-posture adjusting on the lumbar zygopophyseal joints as evaluated by magnetic resonance imaging: a before and after study with randomization. J Manip Phys Ther, 2000;23:380.
Nansel DD, Peneff A, Quitoriano J. Effectiveness of upper versus lower cervical adjustments with respect to the amelioration of passive rotational versus lateral-flexion end-range asymmetries in otherwise asymptomatic subjects. J Manip Phys Ther, 1992;15:99-105.
Nansel D, Waldorf T, Cooperstein R. Time course effect of cervical spinal adjustments on lumbar paraspinal muscle tone: evidence for facilitation of intersegmental tonic neck reflexes. J Manip Phys Ther, 1993;16:91-95.
Lehman GJ, McGill SM. Spinal manipulation causes variable spine kinematic and trunk muscle electromyographic responses. Clin Biomech, 2001;16:293-9.
Childs JD, Fritz JM, Flynn TW, et al. A clinical prediction rule to identify patients with low back pain most likely to benefit from spinal manipulation: a validation study. Ann Intern Med, 2004;141:920-928.
Cleland J, Fritz J, Whitman J, et al. The use of a lumbar spinal manipulation technique by physical therapists in patients who satisfy a clinical prediction rule: a case series. J Orthop Sports Phys Ther, 2006;36:209-214.
Senna M, Machaly S. Does maintenance spinal manipulation therapy for chronic nonspecific low back pain result in better long-term outcomes? Spine, 2011 Aug 15; 36(18):1427-37.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.