How Spinal Manipulation Activates Segmental Stabilization of the Spine
Malik Slosberg, DC, MS
The high-velocity, low-amplitude (HVLA) thrust of a spinal adjustment/manipulation has been documented to have many beneficial effects mechanically and neurologically. Recent studies have explored the impact of the HVLA thrust on the ligamentomuscular reflex and the resultant activation of the multifidus muscle in response to the sudden stretch of local spinal ligaments, joint capsules and intervertebral discs. This reflexively mediated, rapid and unconscious stabilizing muscular response is a protective reaction to the abrupt stretch in order to prevent disruption of molecular bonds in the connective tissue matrix.
The neuromuscular neutral zone, the ligamentomuscular reflex, creep deformation, microdamage of collagen fibers and the role of the multifidus muscle in providing dynamic stability were all reviewed in my last article, "The Neuromuscular Neutral Zone, Dynamic Stability, and Injury/Pain in the Course of Everyday Activity." (June 3 DC) Now let's discuss how the chiropractic adjustive thrust affects these processes in beneficial ways.
Understanding the Impact of the HVLA Thrust on the Multifidus Muscle
In order to understand the impact of the HVLA thrust on multifidi, a review of a study performed on humans undergoing lumbar surgery is necessary.1 After an incision had been made over the involved lumbar segments and while the multifidi were still intact and not yet retracted off their origins on the spinouses and laminae, the supraspinous ligament at L2-3 and L3-4 was electrically stimulated.
The researchers observed that electromyographic recordings (EMGs) from the multifidus muscle demonstrated a direct relationship of muscular contraction in response to receptor stimulation in the supraspinous ligament. The authors explained that electrical stimulation of the supraspinous ligament mechanoreceptors (MRs) resulted in a ligamentomuscular reflex that caused the multifidus to contract in order to stabilize the supraspinous ligament and prevent possible over-distraction and ligament injury.
A 2010 paper2 added that the reflex contractions of multifidus and longissimus can be elicited by electrical stimulation of afferents in discs, capsules and ligaments. The discussion noted that the reflex response is greater when afferents in several tissues are stimulated simultaneously, but mentioned that reflex activation of multifidus (MF) may be initiated just by stretching the supraspinous ligament, suggesting the presence of a discrete ligamentomuscular reflex.
Moving One Bone Relative to Another Activates the Multifidus
The Solomonow paper1 described ligaments as having only a minor mechanical role in maintaining spine stability and emphasized that the muscular co-contraction of anterior and posterior muscles is the major stabilizer of the spine. Importantly, as the authors elaborate, spinal ligaments are endowed with sensory receptors and are situated in key locations sensitive to relative motion of the vertebrae, so their receptors can monitor movement and activate muscles via spinal neurons to maintain or restore stability. Stimulation of these receptors elicits reflex activity in the paraspinal muscles and contributes to maintaining spinal stability when subjected to stress.
The paper concluded that a reflex arc exists in the human spine from MRs in spinal ligaments, discs and facet joints to the multifidi and possibly other muscles. This reflex is triggered at low to moderate loads that cause relative motion of two vertebrae, causing multifidi to become active. Certainly, this description of a reflex triggered by the noninjurious application of force which causes relative motion of two vertebrae sounds decidedly familiar to practicing chiropractors. Furthermore, the paper concluded that when conditions that challenge spinal stability are detected, such as the application of a HVLA thrust, the motor control unit activates appropriate muscles to protect, restore or avoid instability.
Eight years later, another study from the same lab3 described the function of the ligamento-muscular reflex as providing a fast dose of increased joint stability when unexpected movement elicits a sudden increase in ligament tension. This very rapid protective reflex (response time: 2.5 to 5 milliseconds) indicates that it is a fast-acting, reflexively elicited motor response to prevent damage to ligaments and joints. Spinal manipulation provides precisely the high-velocity, yet noninjurious stretch of ligaments that stimulates MRs to reflexively activate the segmental stabilizing multifidus to unload rapidly stretched ligaments and joint capsules.4
Scientific Basis for Understanding the Influence of the Manipulative Thrust
The findings of the above studies provide a scientific basis for understanding one of the major effects of the HVLA thrust applied to dysfunctional joints. In essence, this is what happens: A joint that is injured, inflamed, degenerated, restricted in motion or painful5 results in reflex inhibition, delayed activation and progressive atrophy of the multifidus muscle innervated by that segment.6 By clinical examination, the chiropractor identifies such a lesion (subluxation / joint complex dysfunction) and then applies a HVLA thrust to the joint.
This high-velocity force rapidly stretches the segmental ligaments, joint capsules, intertransversarii and interspinales muscles, and intervertebral discs, and intensely stimulates their numerous stretch receptors. This results in ligamentomuscular reflex activation of the multifidus, which attempts to stabilize the joint and protect it from possible injury as a result of the high-velocity stretch. The segmental multifidus, which has been reflexively inhibited and is atrophying, is stimulated to contract. This may reverse the reflex inhibition, progressive atrophy, and delayed muscle response documented to occur in the segmental multifidus which overlies a dysfunctional joint; and restore dynamic function and contractility to this primary joint stabilizer.7
Reprinted from Brenner AK, Kiesel KB, Buscema CJ, Gill NW. Improved activation of lumbar multifidus following spinal manipulation: a case report applying rehabilitative ultrasound imaging. J Orthop Sports Phys Ther, 2007;37(10):613-619, published online 29 May 2007. doi:10.2519/jospt.2007.2470. Reprinted with permission from JOSPT and its publishers, the Orthopaedic and Sports Physical Therapy sections of the American Physical Therapy Section (APTA).
A Case Report: Post-Manipulation Improved Multifidus Function
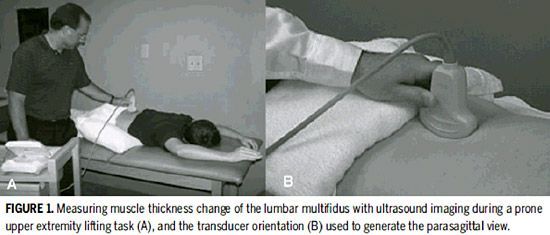
A case report8 of a 33-year-old man with a 21 year history of LBP and posterior thigh pain of insidious onset demonstrated this reflex activation and improved contractility of a segmental multifidus after spinal manipulation. When performing a prone upper-extremity lifting task before manipulation, the patient exhibited a reduced ability to contract his contralateral lumbar multifidus muscle, determined by objectively measuring the pre- and post-manipulation change in multifidus thickness using a validated rehabilitative ultrasound imaging approach.
However, on repeat imaging immediately after and 24 hours after spinal manipulation, thickness change during multifidus activation while performing the prone upper-extremity lifting task increased dramatically. Pre-manipulation thickening with contraction of the multifidus during the prone upper-extremity lifting task demonstrated only a 3.6 percent average change in thickness of the multifidi at L4-L5 and L5-S1, which is well below the 22 percent average increase in asymptomatic subjects. However, after spinal manipulation, there was an immediate increase in MF thickness (17.2 percent) during the upper-extremity lifting task at both L4-5 and L5-S1. This improvement was maintained and slightly increased 24 hours post-manipulation to 20.6 percent.
The pre-manipulation thickness change represents gross muscle dysfunction, but post-manipulation changes approximate normal. The improvement of dynamic muscular function post-manipulation were accompanied by clinical benefits as well. The authors conclude that the change in contractility of the multifidus observed on ultrasound imaging demonstrates possible neurophysiologic/reflexogenic effects of spinal manipulation on the multifidus muscle. As the authors interpret the findings, spinal manipulation may affect the inflow of sensory input to the central nervous system and evoke paraspinal muscle reflexes which alter central and/or peripheral neural pathways.
The Unique Effects of High-Velocity, Low-Amplitude Force
This research, along with many other studies, confirms that dysfunctional spinal joints result in inhibition and progressive atrophy of the local multifidi. This leaves the involved spinal segments unprotected, relatively unstable, and biomechanically vulnerable to injury and recurrences with minimal or no external mechanical load or stress. The application of the high-velocity, low-amplitude force of spinal manipulation generates a rapid stretching of the ligaments, joints capsules, discs and small intrinsic spinal muscles, resulting in a reflex response in the multifidus. The multifidus is reflexively activated and contracts in a region where it would otherwise be losing cross-sectional size and density.
Somehow, based on decades of clinical experience, chiropractors have observed improvements in joint function and intuitively sensed, long before the research was available, that manipulation may help reset disturbed motor programs and activate these key segmental stabilizers in regions where they are inhibited and atrophying. The findings reported above and their practical application to chiropractic care should serve to increase clinicians' confidence in and understanding of the mechanisms and benefits unique to the specific high-velocity, low-amplitude forces produced by spinal manipulation.
Seaman D, Winterstein J. Dysafferentation: a novel term to describe the neuropathophysiological effects of joint complex dysfunction. JMPT, 1998;21(4):267-80.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.