Isthmic vs. Degenerative Spondylolisthesis: Using the "Wide Canal Sign"
Deborah Pate, DC, DACBR
Spondylolisthesis is generally defined as the anterior shift of one vertebral body on another (the segment below it). It is a well-recognized disorder that can cause lower back pain and radiculopathy. Two of the more common causes for a spondylolisthesis are degenerative joint disease of the lumbar facets, allowing anterior slippage of the vertebral body in relation to the one below; and a defect in the pars interarticularis.
Generally, oblique views are performed to visualize the pars interarticularis if there is a spondylolisthesis. Sometimes, however, the oblique view is not helpful because of marked degenerative facet changes that obscure the pars. The cause of the spondylolisthesis needs to be determined because the clinical management will be different, depending on the cause.
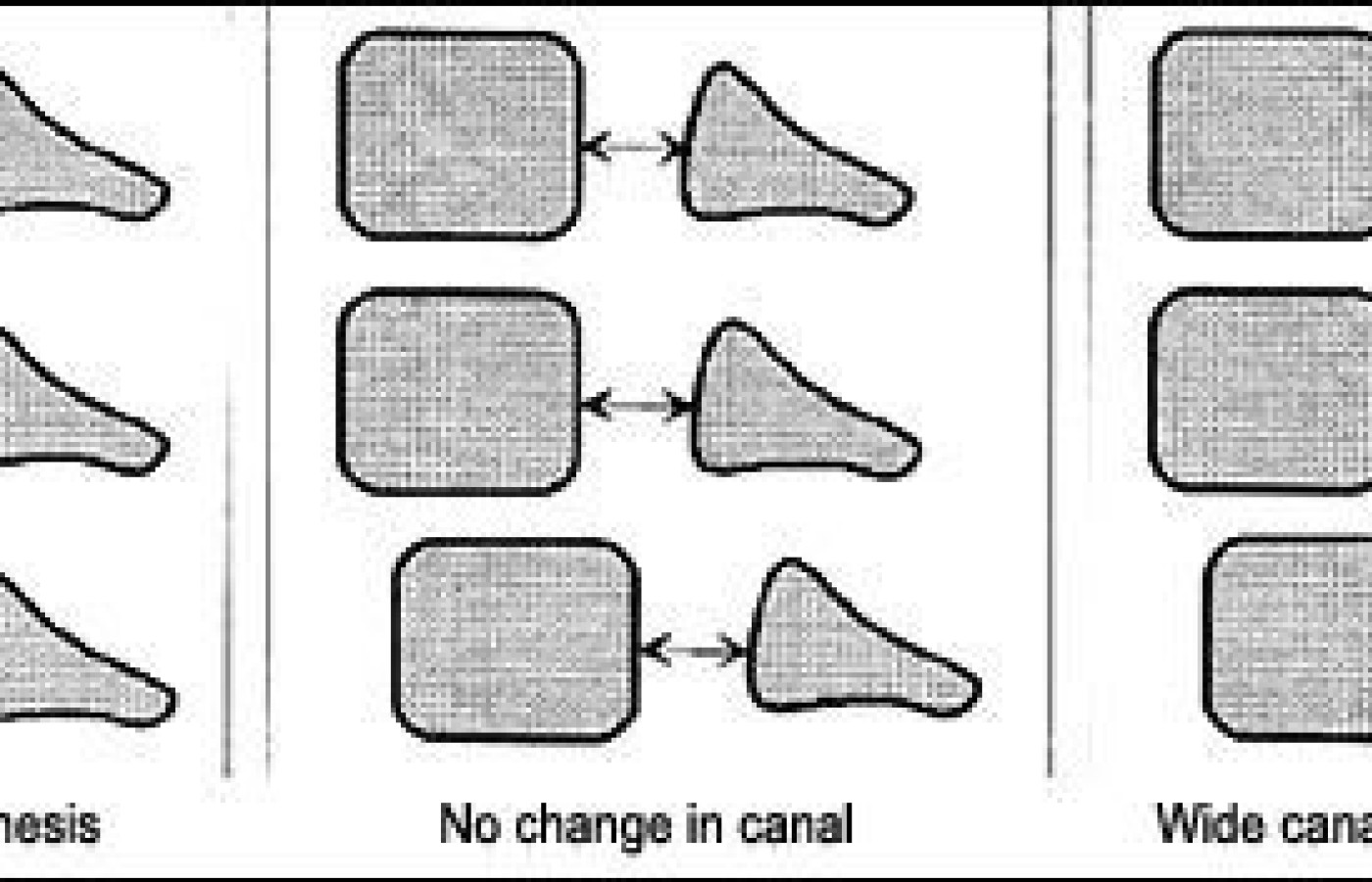
By using the simple anatomic concept that a spondylolisthesis associated with a break in the pars will demonstrate an increase in the sagittal diameter of the spinal canal, the two etiologies can be differentiated. Using the lateral view, determine the diameter of the spinal canal. A simple method is to use the middle of the posterior margin of the vertebral body and the spino-laminar junction as an estimate of the spinal canal, and compare the level with the spondylolisthesis and the adjacent levels. If there is no significant change in the measurement, it is unlikely that a pars defect is causing the spondylolisthesis (see figure above).
This concept is just a guide for determining if there is a lysis of the pars. Further imaging may be necessary to determine if there are other complications, particularly with marked degenerative changes.
Just as a caveat, there is an additional test you can use to determine whether there is anterior spondylolisthesis. This is the right-angle test. An angle is drawn perpendicular to the anterior margin of the sacrum and along the superior margin of the sacrum (see example below).
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.