Chiropractic Cervical SMT and Degenerative Processes
Nancy Molina, DC, QME, MBA, CCSP, Esq.
Objective
Chiropractic cervical spinal manipulation (CSMT) offers the promise of maintaining motion of the spinal unit after loss of lordosis and degenerative processes have occurred to the vertebral, facetal and uncinate joints. The impact of CSMT on sagittal alignment of the spinal unit needs to be addressed, along with its effect on overall sagittal balance of the cervical spine in a postural or biomechanical relationship of function to structure. CSMT improves outcomes in the presence of cervical spinal degenerative joint disease in a chronic neck pain patient.
Methods
The author retrospectively reviewed radiographic and clinical outcomes in a patient who received CSMT, and for whom early (initial baselines at start of care) and late (four months) follow-up data were available. Static radiographs were measured by hand to determine the angle of the cervical curve. Special consideration was applied to avoid retraction or lowering of the chin when obtaining the radiographs, as the effect would straighten the lordosis. Range of motion (ROM), in this case, cervical extension seated, was determined by the use of a goniometric tool in three successive trials; the average finding was utilized. Clinical outcomes were assessed using the Neck Disability Index (NDI) and Dartmouth COOP General Health questionnaires.
ROM was improved following CSMT, with a mean of 8.0 degrees, which was not significantly different from the discharge summary value of 9.0 degrees. When compared with the pre-CSMT angle of the cervical curve, the angle in the neutral position became lordotic in the early and late post-CSMT periods (mean change of 8.0 degrees at the discharge follow-up). There was no statistical correlation between the NDI and Dartmouth COOP outcomes and cervical lordosis that the author was able to determine. The outcomes from baseline to interim to discharge follow-up yielded appreciable improvement in general health that included daily and social activities, and overall health and pain status. The NDI at baseline yielded 24 percent, or moderate disability, whereas discharge findings yielded 5 percent, or mild disability.
Conclusions
CSMT may improve motion of the spinal unit or facetal joints that impart motion segmental to the spinal unit. CSMT improves the clinical outcome of a cervical degenerative joint process, as demonstrated by the NDI and Dartmouth COOP outcomes.
Case History
The patient is a 34-year-old, right-handed female with complaints of chronic pain in the neck. The history of the patient's present illness includes a low-impact motor vehicle accident seven months prior, during which she was rear-ended while at a complete stop. She developed headaches and consequently was seen immediately by a doctor of chiropractic. She was treated with chiropractic manipulative therapy, which offered some improvement of pain. No diagnostics or responses to care were obtained. She developed weakness and clicking in her neck. She tried massage at another chiropractic facility, with some relief. The patient self-discharged from both massage and chiropractic care after two months. She presents on referral from an existing patient.
No past medical history for surgeries. Accidents: reported work-related injury to low back with a C & R or release of future medical for a cash settlement, approximately eight years ago. Auto injury as a passenger involved in low-impact lateral impact, approximately six years ago.
Review of Systems
HEENT: heavy head sensation; denies diplopia or difficulty swallowing. Lungs: negative. Heart: negative. GI: negative. Endocrine: cramping on menses. Musculoskeletal: neck pain on motion and worse at end of day. Limited movement in low back during first morning hours. Poor sleeping habits due to pain. Neurological: none. Psychiatric: negative. Height: 5' 4" tall. Weight: 140 pounds.
Family history is unremarkable. Social history: single, never been married, no significant other. Occupation: biologist for five years. Denies use of tobacco, coffee, alcohol and other drugs. The patient walks for exercise.
Review of Studies
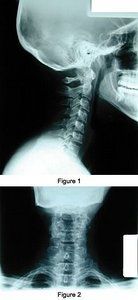
Limited cervical studies (AP and lateral) were obtained at this facility at time of history and physical. Diagnostic yield includes cervical lordosis nonmaintained with alordosis, facetal sclerosis, and cervical spondylosis at C5 and C6. AP view: uncinate processes and adjacent fossae show projecting osteophytes and sclerosis. The soft-tissue structures are unremarkable and bone density is adequate. There is no evidence of any frank osteolytic or osteoblastic findings, congenital findings or obvious fractures (figures 1 and 2).
Physical examination: English-speaking, well-nourished, well-developed, pleasant female in some antalgic distress involving the head and neck. Cervical active ROM was limited on extension and flexion due to pain avoidance and with pain on resisted cervical ROM, extension greater than flexion. Neurological evaluation demonstrated alert mental status; cooperative. Motor 5+. Deep tendon reflexes 3+ except for triceps tendon jerks 2+. Sensory examination reveals hypoesthesia C4, C5 dermatome. Present to light touch, pinprick and vibration. Chiropractic evaluation for soft-tissue palpation yielded some hypertonicity of anterior cervical flexors. Osseous palpation yielded ASRP at atlas, PLS spinous at axis and PR spinous at C5-C7. Joint play/motion palpation painful biaxial splinting at facetal region lower cervical and at midrange of cervical motion. Fixations were present associated with these regions.
Impression
cervical strain - cervical alordosis;
cervical sprain chronic facetal capsular injury; and
chronic facetal osteoarthrosis with uncinate osteoarthrosis (evidenced by radiographic study).
Plan
Monitor neurological and consider possible neurology evaluation.
Possible MRI cervical spine without contrast to rule out HNP cervical C5/C6.
Return in two days for chiropractic physical medicine and rehabilitation care 3x/week x 4 weeks initially. Patient written and informed consent signature and patient baseline outcome assessment forms signature to be obtained at next follow-up visit for counseling on findings and chiropractic care plan. Obtain new outcomes at interims.
Chiropractic technique: diversified and diversified non-force technique (DNFT).
Chiropractic rehabilitation: Pre-adjustive therapies: cervical traction progressive static 15-30 minutes to increase mobility of arthritic complaint, and reduce fibrotic soft tissues - up to four sessions. Pulsed ultrasound trigger-point action to trapeziums, splenius cervicis hypersensitive areas for deeper penetration and relaxation soft tissue x 10 minutes - up to 4-6 sessions. Hydrocollater local heat pack cervical spine x 10 minutes to decrease myospindle response to stress and increase lymph flow. Postadjustment end in topical cryotherapy analgesic gel to cervical region at each CSMT session.
Discussion
The patient completed approximately 26 chiropractic care sessions during the rehabilitative stage in care and only required four sessions for the acute (pain) stage, whereas she received a total of 30 sessions related solely to her neck complaint. She completed follow-ups at one month, two months and six months post rehabilitative chiropractic care. Her final session included a discharge summary that provided instruction and recommendations to seek CSMT at a minimum of once a month to keep discharge disability outcome levels to a minimum.
Cervical extension induces motion that stretches the capsule and its periarticular tissue in directions not specially addressed with rotation or lateral flexion adjustments. Therefore, extension restrictions (flexion malpositions) are more effectively addressed by adjustive techniques and vectors directed specially for this dysfunction. Extension adjustments may be directed to reduce unilateral or bilateral segmentation joint fixations.
The primary chiropractic technique employed in this case study placed the patient in either supine or prone position, and contract was established on the side of restriction over the posterior aspect of the cervical articular pillar. The thrust was gentle and caution was emphasized to avoid joint compression. The atlanto-occipital restriction in flexion (extension malpositions) was treated with methods directed at inducing long axis distraction of the occipital condyle. Conversely, atlanto-occipital restriction in extension (flexion malpostions) was treated with methods directed at inducing anterior-inferior glide of the occipital condyle. This thrust was mainly in the sagittal plane, with some lateral flexion to isolate the joint. Pre-CSMT adjustment assessments were determined and recorded at each patient encounter.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.