Older patients with lower back and hip complaints are not uncommon to our daily practice. We should know if any of our patients have undergone any total joint replacements, since there are problems of concern associated with joint replacements. The most common joint to be replaced is the hip. Patients with lower back pain, with or without hip pain, who have total hip replacements should also be evaluated in regards to their hip replacement, mainly for possible loosening.
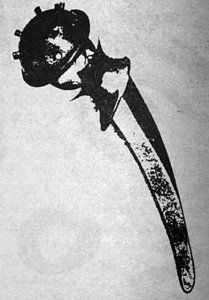
There are two basic types of Total Hip Replacement Arthroplasty (THA). One type is a metallic acetabular component which is cemented in place, and the other is a metallic acetabular component which is not cemented but has metal protrusions on the acetabular side that fix it to the acetabular bone. (Figures 1 and 2)
Figure 1: Mc-Kee Farrar (THA) is a metal-metal articulation. The acetabular component demonstrates the protrusions that result in fixation.
Figure 2: Charnley (THA), ultra high, molecular weight polyethylene grooved acetabular cup for cementing into the acetabulum with a metallic femoral component.
There are several complications associated with THA, which include dislocation, trochanteric avulsion or nonunion, heterotopic ossification, fracture and loosening, or infection. Dislocation is an uncommon complication which occurs within the first few weeks following surgery, which is usually easily diagnosed. Trochanteric avulsion or nonunion is usually assessed within the first six months postoperative.
Heterotopic ossification is a common sequela of THA. The incidence varies from 15 to 50 percent. Mild degrees of heterotopic ossification generally cause no clinical disability. A certain percentage of patients will develop extensive ossification resulting in limitation of motion.
Fractures of the femur and the pelvis may occur intraoperatively and most are recognized at the time of surgery. Postoperative femoral fractures are of two types: a fracture of the femur following major trauma, commonly associated with serious auto accidents. The other type of fracture of the femur can occur spontaneously or following minor trauma. Common areas for these types of fractures to occur are at the tip of the femoral stem, areas where cortical thinning has occurred due to the initial reaming of the intramedullary canal, misdirected screw holes, and areas of inadequate distribution of bone cement. Fractures of the acetabulum can also occur due to over-reaming of the acetabulum, severe protrusio acetabuli, chronic loosening or infection with increased stresses, and perforation of the medial wall of the acetabulum during surgery. Stress fractures can also occur at the pubic ramus in patients that are osteoporotic.
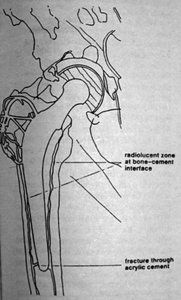
Loosening and infection are the chief long-term complications of the THA and are the main problems that we, as chiropractors, should be aware of. Loosening of a prosthetic component at the bone-cement interface may occur with or without associated infection. Conversely, deep infection is not always associated with component loosening. The incidence of deep infection has decreased in the past decade due to stringent prophylactic measures. There can, however, be a long latent period -- up to eight years in some patients, with deep sepsis. Prosthetic loosening, usually can be revised with success if there is no infection. Infected components generally need to be removed. Unfortunately, the distinction between loosening and infection may be difficult, even with the use of multiple modalities, including x-rays, radionuclide scanning, hip aspiration, and subtraction arthrography. In general, if there is evidence of a radiolucent zone at the bone-cement interface which is 2 mm or wider, infection and/or loosening is a definite possibility. (Figure 3)
Figure 3: Diagram illustrates the most common areas of loosening of the femoral component.
This finding is extremely important to evaluate and follow-up is required if there is any question regarding the bone-cement interface. Loosening of a prosthetic component not only can be associated with pain, but can result in fracture and dislocation depending on the location of the loosening. Care should be exercised when manipulating these patients once we have ruled out any associated problems due to the THA. If the patient is very osteoporotic, I would recommend avoiding any type of chiropractic adjustment that would place stress upon the hip joint or femur, as in a lumbar roll. Basically, to avoid any possible problems with patients that have a THA, it would be prudent to assess the pelvis and the involved hip with a simple x-ray of the pelvis and a view of the hip to include the distal most aspect of the stem of the femoral component. Comparing the present films with previous films can also be helpful if loosening or infection are suspected. If loosening or infection are suggested on the radiographic studies, make certain to follow up with an orthopedic consultation.
References
Resnick and Niwayama. Diagnosis of Bone and Joint Disorders. Saunders 1981.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.