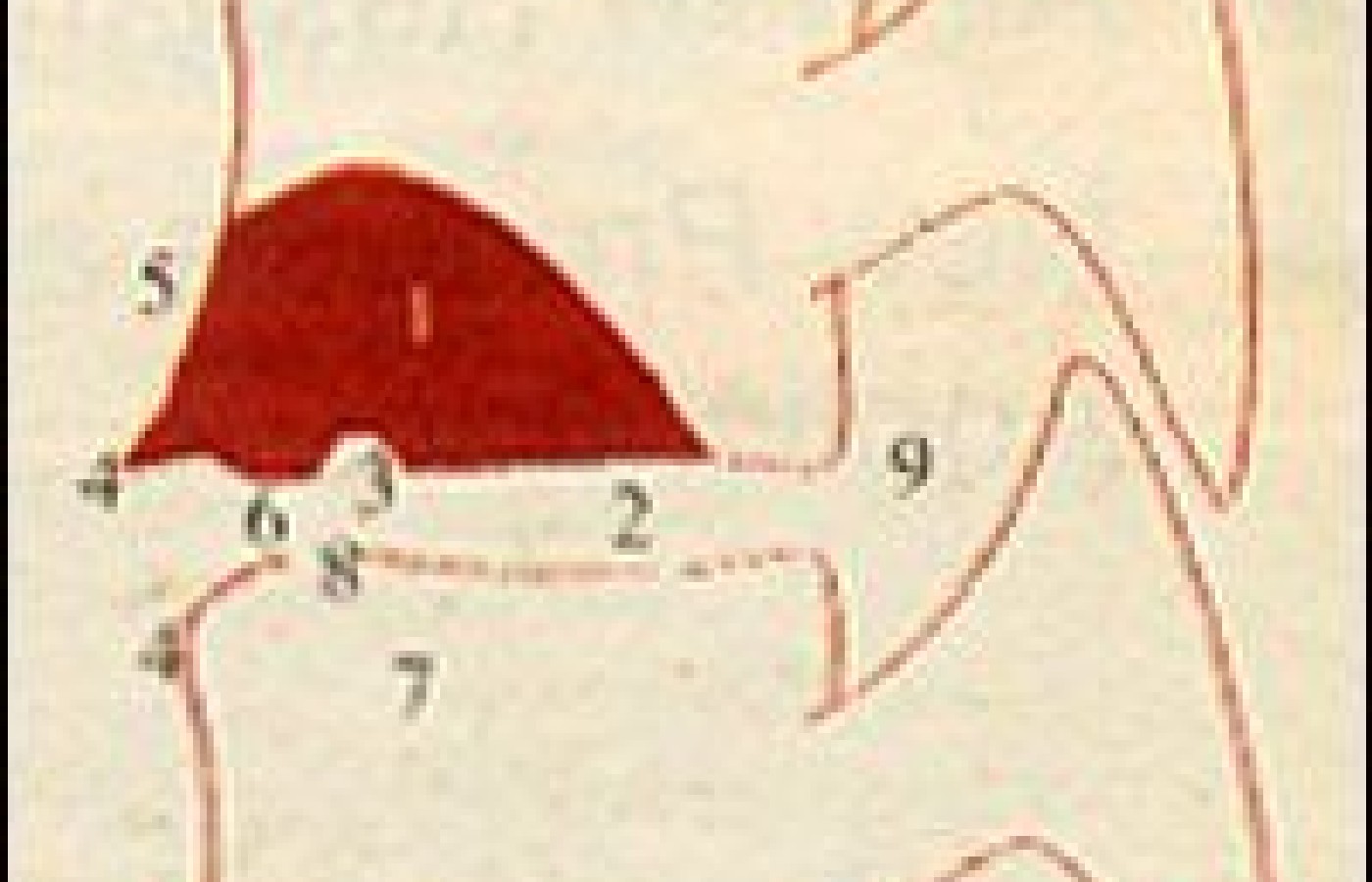
Hemispheric spondylosclerosis has on frequent occasion been confused with more life threatening diseases such as metastatic carcinoma, lymphoma and, less threatening but clinically significant, osteoid osteoma. Hemispheric spondylosclerosis presents radiographically as an increase in the vertebral density resembling a dome or helmet as the vertebral body above or below the intervertebral disc space. The convex area of increased density is located usually in the anterior or middle third of the vertebral body. The convex shape of the sclerosis is always preserved.
In 50 percent of the cases, the L4 vertebral segment is affected. Most of the time a periosteal reaction or a circumscribed ossification of the anterior longitudinal ligament develops where the sclerotic region meets the anterior margin of the vertebral body.
Another common finding associated with this entity is that a small erosion can form at the base of the spherical sclerosis. This is apparently due to the extrusion of disc material into the brittle and sclerosed vertebrae. Eight percent of patients with hemispheric spondylosclerosis develop osteophytes on the anterior aspects of the vertebral body. Most cases demonstrate a decrease in height of the adjacent disc space. I has also been reported that nearly 30 percent of patients with hemispheric spondylosclerosis present with a spondyloretrolisthesis.
It is generally accepted that hemispherical spondylosclerosis is due to degenerative disc disease and the subsequent subdiscal sclerosis of the cancellous bone. It constitutes an adaptive thickening of the cancellous trabeculae which develops as the result of the decreased elasticity of the degenerative disc.
Distribution of features of hemispheric spondylosclerosis of the spine:
Typical hemispheric or helmet shape of hemispheric spondylosclerosis with its center in the anterior portions of the vertebra or, less frequently, expanding into the posterior third of the vertebral body -- 100 percent.
Decrease in disc height --87 percent.
At least one very small erosion in the base of the sclerosis -- 85 percent.
Vertebral osteophyte(s) -- 81 percent
Smooth or denticulate periosteal reaction at the anterior contour of the vertebra or ossification of the anterior longitudinal ligament along the sclerosis -- 79 percent.
Caudally directed new bone formation at the anterior base of the sclerosis -- 74 percent.
Multiform spondylosclerosis of the subjacent vertebra -- 64 percent. (Hence in 36 percent of the observations this infradiscal spondylosclerosis was absent.)
Erosion(s) in the region of the intradiscal end-plate -- 36 percent.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.