Infrared Thermography and the Sports Injury Practice
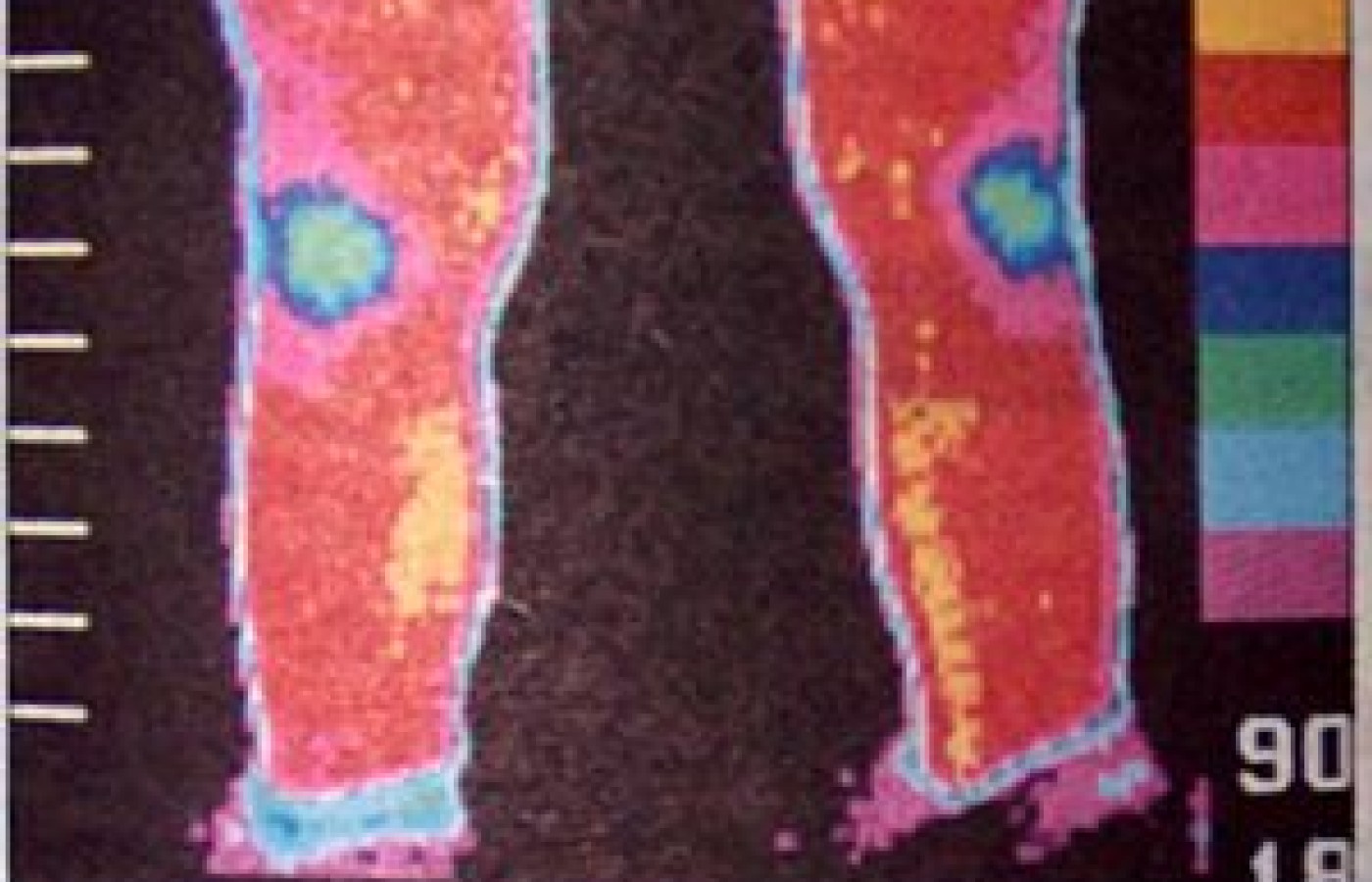
Infrared thermal imaging can be very useful to the sports injury practice. Infrared Thermography (IRT) measures cutaneous surface temperature which is reflective of the underlying sympathetics and local chemical mediators. Previous studies have shown that skin temperature from right to left sides only differ within a few tenths of a degree for homologous parts. In the case of the anterior calves, the normal mean temperature differential is .31 degrees C. Other studies have shown that temperature differentials over .65-.80 degrees C are indicative of underlying pathology. IRT has been found to be useful by both the AMA Council on Scientific Affairs and the ACA Council on Diagnostic Imaging, which has its own American Chiropractic College of Thermology.
IRT has been documented in the world scientific literature as an efficacious diagnostic tool, prognostic and treatment assessment tool. IRT has been shown to be useful for stress fractures, tibial stress syndromes (shin splints), patellofemoral disorders, shoulder impingement, reflex sympathetic dystrophy, Osgood Schlatter's disease, epicondylitis, nerve entrapments, ankle injuries, foot disorders, and myofascial pain syndromes. In a study published by Goodman, et al., IRT was found to be a useful test to distinguish stress fractures and shin splints in a prospective blind study of runners. The athletes with hyperthermic calves had a poorer prognosis as opposed to those with a hypothermic/cold pattern. In a study by this author that was presented at the 17th Annual Symposium of the American College of Sports Medicine, and to be published in the JMPT, IRT was found to have a high sensitivity and specificity for patellofemoral pain syndrome (PFPS). PFPS will image as a global patellar hypothermia that will usually affect the patella region only.
IRT is useful in the differential diagnosis of knee disorders since PFPS will typically image the knee as cold, and meniscal injuries will typically image hot or hyperthermic. IRT has also been documented to be useful for epicondylitis. In a study by Binder, et al., 53 out of 56 patients showed a characteristic focal hyperthermia over the involved elbow and epicondyle. The hyperthermic finding is characteristic of a somatocutaneous reflex response. While IRT is not necessary as a diagnostic tool for ankle sprains, it is extremely useful as a prognostic and assessment tool to predict the course of the injury. Hyperthermic ankle sprains heal in the usual time frame; however, cold pattern ankle sprains take much longer and have a poorer prognosis with relapses if allowed to return to competition too soon. IRT has been found to be useful in entrapment neuropathies such as carpal tunnel syndromes and ulnar neuropathies which are not uncommon in cyclers. One of the biggest contributions of IRT is in the area of reflex sympathetic dysfunction (RSD) which is characterized by three different stages and often occurs after minor injuries and traumas or post-surgical. Stage I is a stage of sympathetic hypertonia and has also been called "sympathetic maintained pain." It is clinically characterized by pain that "does not go away," burning, allodynia, hyperalgesia, vasomotor and sudomotor dysfunction. If it is undetected or not treated properly, it can progress to Stage III which then can cause dystrophic changes to bone, skin, and muscle. RSD should be especially thought of when dealing with chronic ankle, shoulder, and knee injuries, or when the patient complains of an extremely cold extremity with burning, allodynia, and hyperalgesia.
IRT is also helpful in the following conditions:
Shoulder impingement syndrome -- focal hyperthermia of shoulder.
Achilles' tendinitis -- focal hyperthermia at Achilles' tendon.
Morton's neuroma/metatarsalgia -- focal hyperthermia at plantar foot.
Tarsal tunnel syndrome -- hypothermia at heel and big toe.
Osgood Schlatter's disease -- focal hyperthermia at tibial tubercle.
Tennis leg -- hyperthermia over head of involved gastrocnemius as opposed to diffuse hyperthermia in phlebitis.
IRT is also useful as a prescan team assessment tool, to determine areas of thermal asymmetry that may represent subclinical problems predisposing the athlete to injury. For example, in a study done by this author, it was found that 70 percent of a high school football team showed patellar thermal asymmetry. IRT can be used with follow-up studies to follow treatment response and as a prognostic indicator of when to best return the athlete to practice and/or competition.
Conclusion
Infrared thermography has many applications in a sports injury practice and is valuable for diagnostic, prognostic, and treatment assessment purposes. Thermography should be utilized whenever possible by sports medicine doctors.
Reference:
Feldman F, Nickoloff E: Normal thermographic standards in the cervical and upper extremities. Skeletal Radiol, 12:235-249, 1984.
Uematsu S: Symmetry of skin temperature comparing one side of the body to the other. Thermology, 1(1): 1985.
Uematsu S, Edwin DH, Jankin WR, Kozikowski J, Trattner M: quantification of thermal asymmetry, Part I. Normal values and reproducibility. J Neurosurg, 69:552-555, 1988.
Goodman PH, Murphy MG, Siltanese GL, Kelly MP, Rucker L: Normal temperature asymmetry of the back and extremities by computer assisted infrared imaging. Thermology, 1:195-202, 1986.
Hobbins WB: Basic concepts of thermology and its application in the study of the sympathetic nervous system. Second Albert Memorial Symposium, Washington, D.C., 1986.
Kellgren JH: On the distribution of pain arising from deep somatic structures with charts of segmental pain. Clinic Sci., 4:35-46, 1939.
Travell JG, Simons DG: Myofascial Pain Dysfunction -- The Trigger Point Manual. Baltimore, Williams & Wilkins, 1980.
Hobbins, WB: Thermography in sports medicine. Sports Medicine ed 3, Appengeller, Schwarzenberger, 395: 1988.
Schmitt M, Guillot Y: Thermography and Muscular Injuries in Sports Medicine, Recent Advances in Medical Thermology. Plenum Press, New York, 439-445: 1984,
Binder AL, Parr G: A clinical and thermographic study of lateral epicondylitis. Br J Rheum., 22:77-81, 1983.
Perelman, RB, Adler, D, Humphreys M: Reflex sympathetic dystrophy: Electronic Thermography as a Diagnostic Tool. Orthop Rev., 16(8):53-58, 1987.
Lewis, R, Racz G, Fabian G: Therapeutic approaches to reflex sympathetic dystrophy of the upper extremity. Clinical issues in Regional Anesthesia, 1(2): 19--.
Devereaux MB, Graham RP, Lachman SM: The diagnosis of stress fractures in athletes. The Physician and Sports Medicine, New York, McGraw Hill, 52:531-533, 1987.
Herrick, RT, Herrick SK: Thermography in the detection of carpal tunnel syndrome and other neuropathies. J Hand Surgery, 12A(5):943-9, 1987.
BenEliyahu, DJ: Thermography in the diagnosis of sympathetic maintained pain. AJCM, 2(2):55-60, 1989.
Leroy PL, Christian CR, Filasky R: Diagnostic thermography in low back pain. Clin J Pain, 1:4-13, 1985.
Pochaczevsky R, Wexler CE, Myers PH, Epstein JA, More JA: Liquid crystal thermography of the spine and extremities. J Neurosurg., 56:386-395, 1982.
Uematsu S, Junkel W: Skin temperature response of the foot to cold stress of the hand: a test of evaluation somatosympathetic response. Thermology, 3:41-49, 1988.
Pochaczevsky R: Thermography in posttraumatic pain. Am J Sports Med., 15(3):243-250, 1987.
Uematsu S, Hendler N, Hungerford D, Long D, Ono N: Thermography and electromyography in the differential diagnosis of chronic pain syndrome and reflex sympathetic dystrophy. Elect Clin Neurophys, 21:165-182, 1981.
David J. BenEliyahu, D.C., D.N.B.C.T., C.C.S.P. Selden, New York
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.