Infrared Thermography in the Personal Injury Practice: An Overview for Whiplash Injuries
Infrared thermography is a valuable tool for doctors treating patients who have sustained personal injuries from auto accidents and slip/fall type accidents. Infrared thermography (IRT) can provide information and objective documentation for soft tissue type injuries like no other test can. IRT is a test of neurophysiology that is useful for myofascial trigger points, radiculopathy, temporomandibular joint (TMJ) syndrome, scleratogenous pain/sprain/facet syndromes, thoracic outlet syndromes, cephalalgias, reflex sympathetic dysfunction, knee disorders, shoulder disorders, nerve entrapment, double crush syndrome, and disc protrusions.
IRT is not only useful for the differential diagnosis but can help the treating doctor monitor patient progress, assess treatment modalities, have an objective measure when the patient reaches maximum medical improvement, rate physical impairment, and define prognosis.
Acceleration/deceleration injuries to the spine will typically affect the patient's central and autonomic nervous system. It has been documented that IRT measures sympathetic dysfunction and that all spinal and peripheral nerves carry 8 percent to 30 percent sympathetic nerve fibers. Right to left symmetry is the expected observation in homologous parts. When there is nerve injury thermal asymmetry will be observed in the extremity dermatomes or thermatomes. If nerve injury is due to direct nerve root compression, whether by large disc herniation, spinal stenosis, or a large spur, a dermatomal pattern of thermal asymmetry will be observed. (Figure 1) If nerve injury is due to irritation, such as by disc herniation or bulge causing sinuvertebral nerve irritation at the annulus with chemical mediators causing nociception as well (PLA2), an "autonomic" pattern of referral will be observed. Likewise, if the facets are sprained, the joint capsule will reflect changes in the sympathetics due to nerve irritation and chemical nociception.
IRT has been documented by many authors to be useful in disc herniation cases. A study done by Chafetz, et al., and published in Spine found 100 percent sensitivity for IRT in CAT scan documented disc herniations. A study by Dale and published in the British Journal of Rheumatology found a 91 percent correlation of IRT and MRI in lumbar disc herniations. Studies published by this author in Manual Medicine, JMPT, and Chiropractic Medicine have found IRT to be useful in both cervical and lumbar disc herniation cases. In a study recently published in Chiropractic Technique, this author found IRT to be useful as a treatment assessment tool for patients with lumbar disc herniations.
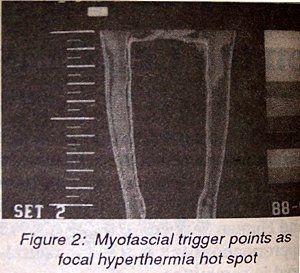
Very often, overlying nerve irritation patterns the patient will also complain of myofascial pain. IRT images myofascial trigger points as a focal hyperthermia hot spot. (Figure 2) Diakow, Fischer, Kruse, Chapman, and others have all documented the clinical utility of IRT in the scientific literature for myofascial trigger points.
Facet syndrome/subluxation or joint sprains will typically image as focal hyperthermia overlying the joint involved. The sacroiliac will image as hyperthermia as well when irritated or sprained. Kobrussi documented the findings of a hyperthermic sacroiliac pattern that resolved after a course of chiropractic manipulative therapy.
TMJ syndromes which are also common in the whiplash injury will be typically imaged as a focal hyperthermia overlying the TM joint and blush hyperthermia over the temporalis and masseter regions. Studies by Weinstein and Steed and recently published in Cranio have documented the clinical utility of IRT in TMJ disorders. IRT is thus useful in differential diagnosis of headache, since TMJ patterns will be different from that of migraine, cluster or tension headache. Cluster headaches will typically yield a "Chai" sign of hyperthermia on the contralateral side; migraines typically yield a supraorbital cold patch on the ipsilateral side. Muscle tension headaches will reveal myofascial irritation patterns that will follow trigger point patterns published by Travell.
Entrapment neuropathies, such as carpal tunnel and ulnar nerve entrapment will show thermal asymmetry in the peripheral nerve field of the involved nerve.
Thoracic outlet syndrome will typically show abnormal findings in the C8/T1 nerve fields and can be especially documented when the patient is stressed with their arms overhead or with a cold stress test.
Autonomic challenge with cold stress test and IRT imaging is very useful to document autonomic and vasomotor instability.
IRT has also been shown to be very useful in documenting the presence of "dashboard knee" which is a patellofemoral contusion and images as hypothermia.
Shoulder impingement or rotation cuff tears will image as a focal hyperthermia.
Reflex sympathetic dysfunction (RSD) which is a condition of sympathetic hypertonia causes global extremity hypothermia in a diffuse pattern. RSD is a serious condition that must be diagnosed early for successful treatment or will otherwise result in a lifetime of misery and disability.
Infrared thermography has good clinical utility, sensitivity, and reliability for the multiple injuries that are encountered in the personal injury practice. IRT is helpful in the differential diagnosis and objective documentation of these injuries.
References
Uematsu S: Quantification of Thermal Asymmetry. J Neurosurg, 69:552-555, 1988.
Goodman PH: Normal Temperature Asymmetry of the Back and Extremities. Thermology, 1:195-202, 1986.
Feldman F & Nickoloff EL: Normal Thermographic Standards for the Cervical Spine and Upper Extremities. Skel Radiology, (12):235-49, 1984.
Pocacheczevsky R, et al: Liquid Crystal Thermography of the Spine and Extremities. J Neurosurg, (56):386-395, 1982.
Wexler C: Overview of Lumbar, Thoracic, and Cervical Thermology. Thermographic Services, Inc., 1983.
Fischer AA: Correlation between Thermographic Findings and SEP in LS Radiculopathy. Thermology (2):29-33, 1986.
Green J & Reilly A: Comparison of Neurothermography and Contrast Myelography. Orthopedics, 9(12):1699-1704, December 1986.
Yuen TS & Aminoff MJ: Clinical Utility of Thermography in Patients with Lumbosacral Radiculopathy. Neurology, (39):376, March 1989.
Hobbins W: Initial. 8(2): Nov. 1987.
Jinkins JR, Whittemore AR & Bradley WG: American Journal of Roentgenology, 152:1277-1289, June 1989.
Bogduk N: Innervation of the Cervical Intervertebral Discs. Spine, 11:873-878, 1988.
Marzo JM: Intradural Connections between Adjacent Cervical Spinal Roots. Spine, 12(10):964-968, 1987.
Chapman G: Cephalic Thermography -- An Overview. Chiropractic Products, June 1989.
Swerdlow B & Dieter J: Validity of the Vascular Cold Patch in the Diagnosis of Chronic Headache. Headache, 26:22-26, 1986.
Chapman G: TMJ Dysfunction and Thermal Imaging -- An Overview. Chiropractic Products, December 1988.
Kellgren JH: On the Distribution of Pain Arising from Deep Somatic Structures. Clinical Science, 4(439):35-46
Mooney V & Robertson: The Facet Syndrome. Clinical Ortho, (115):149-156, 1976.
McCall W, Park WM & O'Birne JP: Induce Pain Referral from Posterior Lumbar Elements. Spine, 4(5):441-446, Sept. 1979.
Wexler C: Atlas of Thermographic Lumbar Patterns. Thermographic Services, Inc., Tarzana, Ca.
McFadden JW: Liquid Crystal Thermography and the Facet Syndrome. J Neurological Orthopedic Medicine and Surgery, 5(4): December 1984.
Chapman G: Biomechanical Impropriety of Intervertebral Motor Units and Thermal Imaging -- Second Opinion. J of the IACT, 1(1): 1988.
BenEliyahu DJ: Thermography in the Diagnosis of Sympathetic Maintained Pain. American J of Chiropractic Medicine, 2(2): June 1989.
BenEliyahu DJ: Thermography in the Diagnosis of Sympathetic Maintained Pain. American J of chiropractic Medicine, 2(2): June 1989.
BenEliyahu DJ: Reflex Sympathetic Dysfunction and Sympathetic Maintained Pain. The American Chiropractor, May 1989.
Lewis R, Racz G & Fabian G: Therapeutic Approach to RSD of the Upper Extremity. Clinical Issue in Regional Anesthesia, 1(2).
Kellgren: The Anatomical Source of Back Pain. Rheumatology and Rehabilitation, 16(1):3-9.
Ravin TH: Thermographic Evaluations of Intramuscular Injections, Second Opinion. Journal of the IACT, 1(1):17, Summer 1988.
Travell J: Myofascial Pain and Dysfunction. William and Wilkins.
Fischer AA: Temperature and Pressure Threshold Measurements in Trigger Points Thermology, 1:212-215, 1986.
Dale, et al: Proceedings of the American Academy of Thermology, May 1989.
Chafetz, Wexler, Kaiser: Neuromuscular Thermography of the Lumbar Spine with CAT Scan Correlation. Spine, 13(8): August 1988.
BenEliyahu DJ: Thermography in Clinical Chiropractic Practice. ACA Journal 26(8): August 1989.
David J. BenEliyahu, DC, DNBCT, CCSP Selden, New York
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.