Spondylolysis and Spondylolisthesis often become confusing. Spondylolysis is a term used to describe a defect in the pars interarticularis or a break in the pars.
The most common level for a spondylolysis is L5. It is rarely found in the cervical spine. It is unilateral in about 1/6 to 1/3 of cases. The cause of a spondylolysis is felt to be repeated trauma, as in a stress fracture, to a par interarticularis that has been inherently weakened by hypoplasia or dysplasia of the pars, most often developmental. The most accepted documented reason for a spondylolysis in young children is torsional stresses or repeated trauma to a hypoplastic or dysplastic pars, ultimately causing a stress fracture. There are however instances when a single traumatic event will cause a spondylolysis.
The best view to determine the presence of a spondylolysis in on the oblique view. If there is a question as to whether or not there is one present, a CT scan will demonstrate this region very clearly. If a possible recent fracture is suspected a bone will demonstrate whether or not the spondylolysis is recent.
Spondylolisthesis is defined as a subluxation of one vertebral body on another; displacement generally is understood that the superior vertebral body is displaced anterior in relationship to the inferior vertebral body.
Spondylolisthesis may be classified as isthmic, degenerative, dysplastic, traumatic or pathologic. In isthmic spondylolisthesis, the cause of the spondylolisthesis is due to a spondylolysis of the pars, and therefore allows the anterior slippage of one vertebrae on another. Dysplastic spondylolisthesis is often due to developmental hypoplasia of the pars, which may be elongated, allowing for the anterior slippage of one vertebrae on another. Traumatic spondylolisthesis is almost always due to a fracture of the posterior arch which allows for slippage of the fractured vertebrae on the adjacent segment. The best example is the "hangman's fracture." Degenerative spondylolisthesis is due to alteration in the biomechanics of the facets, which generally demonstrated marked degenerative changes and allow for the spillage of one vertebrae on another. Neoplastic processes can cause destruction of a vertebral body, again allowing for the displacement of one vertebrae on another, which is termed a pathologic spondylolisthesis.
It is important to note what type of spondylolisthesis is present for clinical management of the patient. There is also a grading system for determining the stability of a spondylolisthesis. This system I am sure everyone is aware of, however, it is more important to determine if there is in fact a progression of the anterior slippage. Any progression of the anterior slippage is even more important than the grade of spondyloslisthesis. If there is radiographic evidence of an increase in the anterior displacement, that alone is enough to document instability.
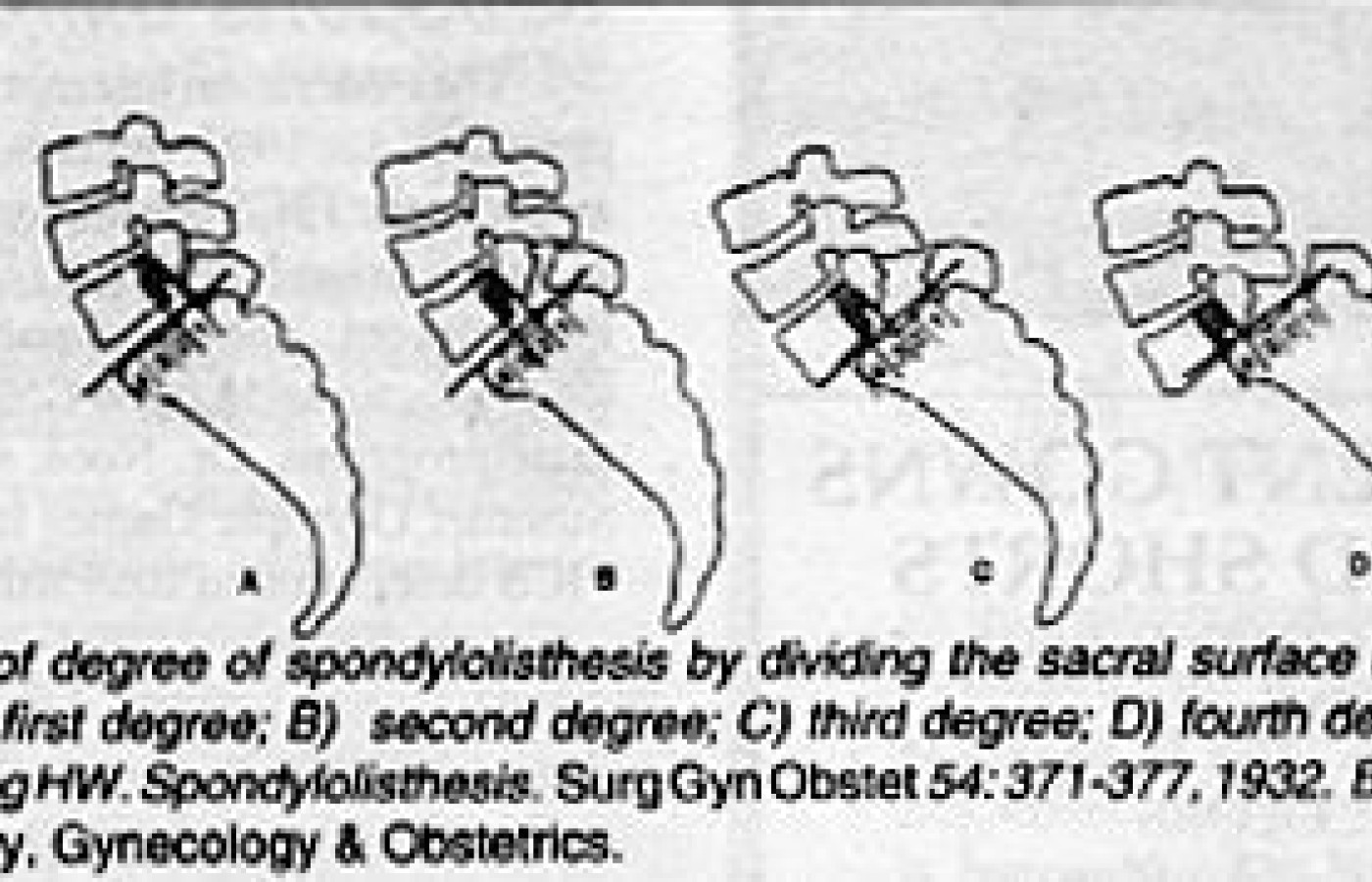
Grading of degree of spondylolisthesis by dividing the sacral surface in four equal parts. A) first degree; B) second degree; C) third degree; D) fourth degree. From: Meyerding HW. Spondylolisthesis. Surg Gyn Obstet 54: 371-377, 1932. By permission of Surgery, Gynecology & Obstetrics.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.