Cubital tunnel syndrome is the second most common entrapment neuropathy of the upper extremity, with reports of problems related to ulnar compression at the elbow dating back more than 100 years.1
The cubital tunnel begins at the medial posterior condylar groove of the humerus at the point where the posterior condylar groove is spanned by the cubital tunnel retinaculum.2 The cubital tunnel retinaculum runs from the medial epicondyle of the humerus to the olecranon and is transversely oriented to the path of the nerve. The cubital tunnel retinaculum may be readily palpated by flexing the elbow and applying finger tip pressure along the path of the posterior condylar groove, because the retinaculum is tightened in flexion and relaxed in extension. The cubital tunnel continues distally, as the ulnar nerve passes between the two heads of the flexor carpi ulnaris muscle and enters the forearm.
Most cases of cubital tunnel entrapment of the ulnar nerve occur between 1.5 centimeters and 3.5 centimeters distal to the medial epicondyle. The cubital tunnel's volume decreases with flexion of the elbow, thus increasing the pressure on the ulnar nerve with this position.3 Pressures greater than 100 mm Hg have been documented to occur with elbow flexion when the cubital tunnel retinaculum is artificially tightened. Paresthesia has been induced within 10 minutes in normal subjects when peripheral nerves are artificially subjected to 50 mm Hg of compression.4 Most cubital tunnel entrapment syndromes are primarily due to compression of the ulnar nerve from the narrowing of the cubital tunnel with flexion of the forearm.
Work related factors may contribute to cubital tunnel syndrome. Complaints of this condition have been associated with computer keyboard operators working all day with the elbows flexed and the ulnar nerve resting on a hard surface. Truck drivers maintaining the elbows in the flexed posture for long periods with the added insult of elbow pressure versus the arm rest may also develop this syndrome.
Secondly, compression from local pathologies may also cause cubital tunnel syndrome by increasing the size of the nerve, decreasing the available space for the nerve by thickening of the cubital tunnel retinaculum, and by bony overgrowth from osteoarthritis. Additionally, the ulnar nerve may be compromised at this site due to local inflammatory swelling associated with rheumatoid arthritis or from the development of space occupying lesions at this site.
Common complaints associated with this syndrome include complaints of aching pain or discomfort at the medial aspect of the elbow and in the proximal forearm which are sometimes associated with shooting pains into the ulnar side of the hand and little finger. Occasionally there may be proximal radiations of pain. Frequently noted symptoms include numbness, tingling, and coldness of the little finger and the ring finger. Occasionally patients may have no noxious symptoms associated with this entrapment neuropathy. Nocturnal symptoms, while very common in carpal tunnel syndrome, are infrequent complaints in cubital tunnel syndrome.
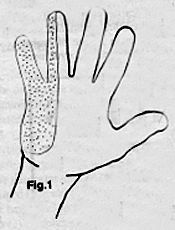
Hypoesthesia in the ulnar field of the hand (Figure 1) may be intermittent or activity related. Activity related hypoesthesia is usually associated with repetitive movements of the elbow or from the maintenance of a constant flexed elbow posture. Motor complaints associated with cubital tunnel syndrome consist of complaints of clumsiness, weakness, and/or dropping of objects. Muscle wasting is primarily noted in the flexor digitorum profundus muscle to the fourth and fifth fingers, the flexor carpi ulnaris muscle, and the ulnar-innervated intrinsic muscles of the hand.
References
McPherson SA and Meals RA. Cubital tunnel syndrome. Ortho Clin North Am, 23:111-123, 1992.
O'Driscoll SW, Horii E, Carmichael SW and Morrey, BF. The cubital tunnel and ulnar neuropathy. JBJS, 73-B:613-617, 1991.
Sunderland S. Nerves and Nerve Injuries, Second Edition, Churchill Livingstone, NY, 1978.
Buehler MJ and Thayer DT. The elbow flexion test -- a clinical test for cubital tunnel syndrome. Clinical Orthopaedics and Related Research, 233:213-216, 1988.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.