Editor's note: A graduate of National College of Chiropractic, Dr. Palo is a professor emeritus at New York Chiropractic College for the DABCO program, and served as assistant director of the New York City Department of Health's chiropractic division.
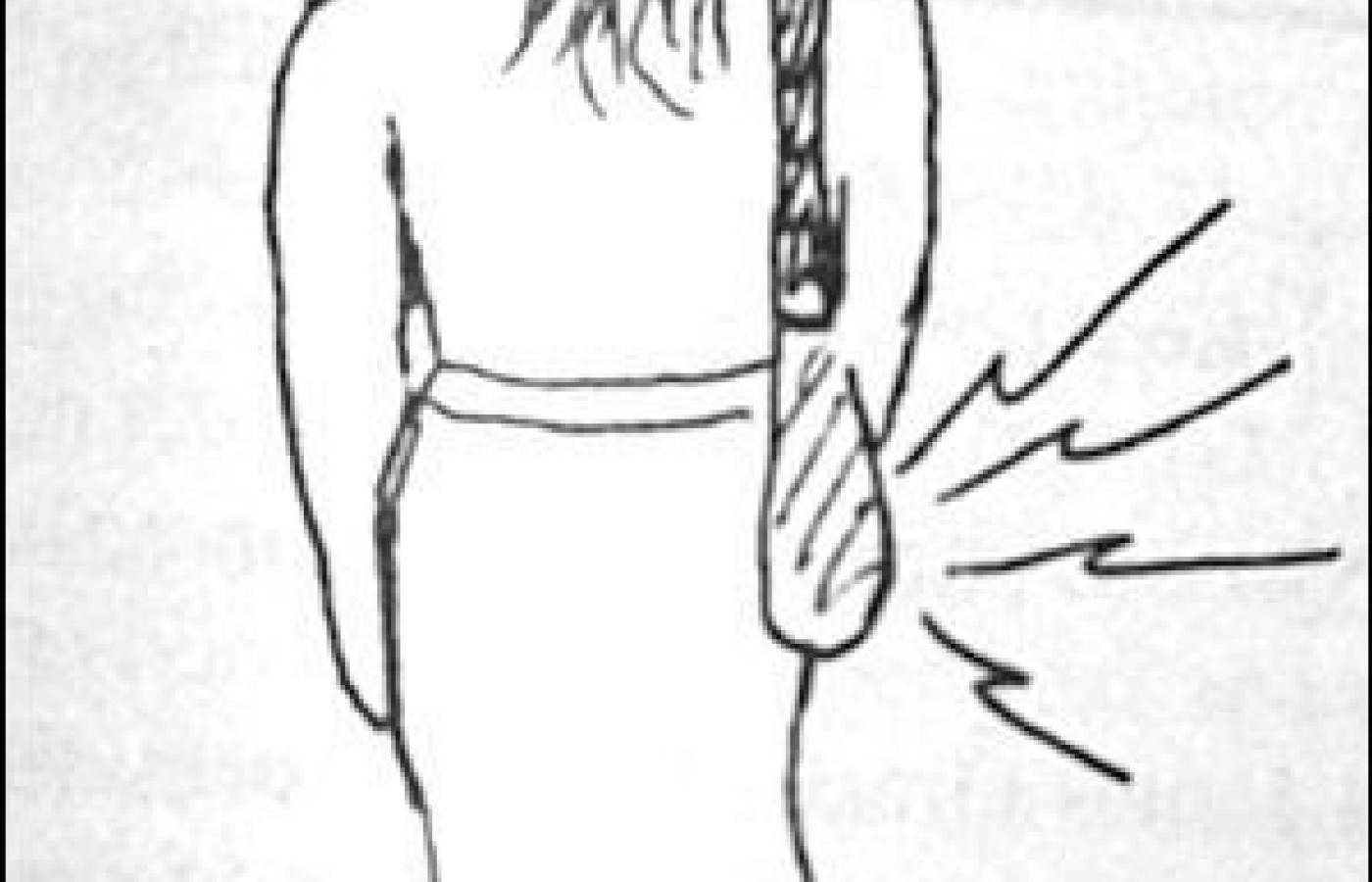
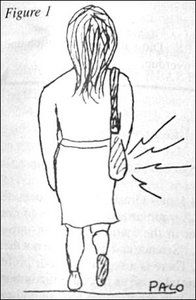
Are you seeing more patients with trochanteric bursitis? This office is. Their history reveals most of them use a shoulder strap carrying bag. We've come to the following conclusion. The bag is hitting upon and irritating at the femur's greater trochanter. Back and forth, as they walk, the bag rubs on the femoral prominence. This continuous irritation soon initiates as inflammation of the bursa overlying the greater trochanter, i.e., trochanteric bursitis.
Diagnosis
That patient presents with an exquisite pain over the involved greater trochanter. It hurts if he sleeps on the involved side. Digital pressure at the greater trochanters elicits much greater pain at the involved side.
In diagnosing trochanteric bursitis we should check for hip osteoarthritis. OA can also present pain in the hip area, especially just above the greater trochanter. A positive Patrick test1 for OA should lead to an x-ray to confirm hip joint osteoarthritis. As in trochanteric bursitis, sleeping on the involved side, in OA, also emits hip area pain. However, the bursitis pain is usually directly on the greater trochanter. It is more pin-pointed, i.e., less dispersed than OA pain.
We may also bear in mind hip OA may also reflect in the groin. Of course, so may a sacroiliac subluxation. However, a trochanteric bursitis will be negative with the Yeoman sacroiliac test2 and will not elicit groin pain.
A Longer Leg
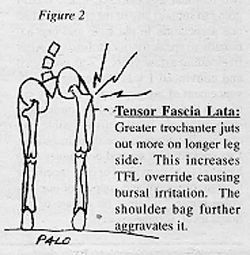
The long leg3 side is more prone to trochanteric bursitis than the shorter leg side. At the shorter leg side the greater trochanter goes lateral and is more prominent. This jutting out of the greater trochanter makes it more vulnerable. Even with no bag rubbing at the long leg's greater trochanter protrusion, this office has found runners prone to longer leg side trochanteric bursitis. This "runner's bursitis" is from repetitive greater override of the tensor fascia lata over the greater trochanter.
Pointed pain at the greater trochanter and a negative Patrick test should provide a good "working" diagnosis of greater trochanteric bursitis. Of course, if a longer leg is present it should be attended to so as to reduce the patient's greater vulnerability on the longer leg side.
Treatment
The immediate treatment for trochanteric bursitis is ice. This should reduce the bursa inflammation.
The patient should be advised to shift the carrying bag to the other side. This stops the cause.
In both hip OA and trochanteric bursitis, patient should refrain from sleeping on the involved side.
Should the doctor discover a long leg contributing factor the patient should be provided a compensatory heel lift for the short leg shoe.
(In viewing hundreds of people walking the streets, this author estimates about one in three are currently using a shoulder strap carrying bag. Unfortunately, the bag usually falls directly upon the greater trochanter. The heavier the bag, the greater the irritation. The greater the irritation, the greater the chance of trochanteric bursitis. As more and more use should strap bags, doctors of chiropractic should be alert to the increasing prevalence of trochanteric bursitis.)
References
Palo, J. Basic Orthopedic and Neurological Tests for the Office. New York, 1994.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.