A seldom attended articulation in the shoulder girdle is the first rib. We motion palpate the heck out of the glenohumeral joint; some of us actually motion palpate the scapula. But how many of us consider the first rib as part of the shoulder girdle? We should.
When the patient has that persistent, nagging, "shoulder pain," that "something not right in the shoulder," the "almost better but ..." shoulder, the "tingling down the arm" shoulder, it is way past time to evaluate the first rib.
What I have found in clinical practice (descriptive research) is that there is a reliable specific sequence to locate, evaluate, and adjust the first rib.
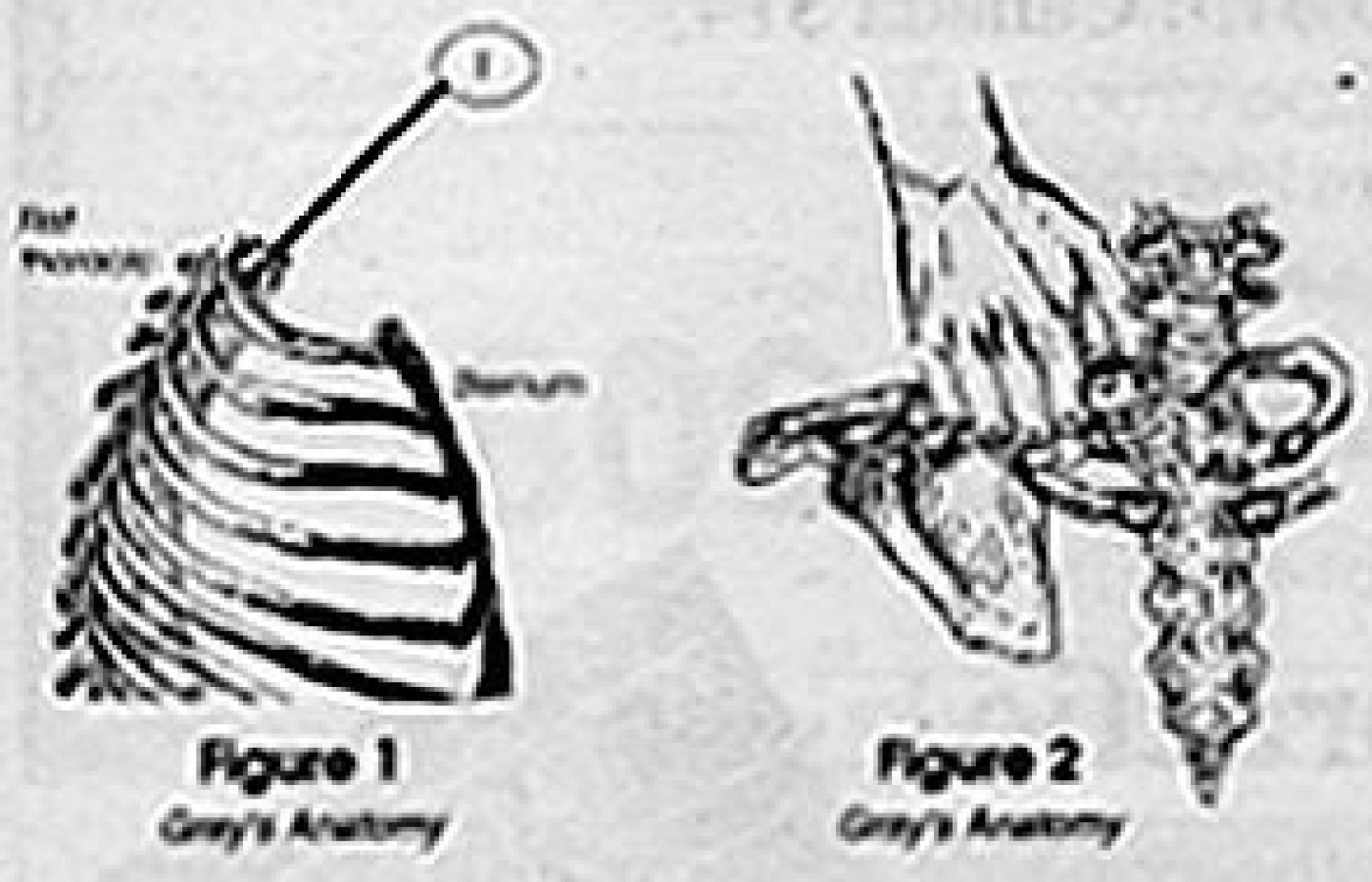
Where Is the First Rib?
Before you can palpate (either static or motion) the first rib you have to know where it is located.
How to Get There ...
Standing behind the patient, place your thumb in front of the trapezius pointing posterior medial with your fingers curled about the clavicle. The suggestion of curling your fingers about the clavicle is to prevent your fingers from resting on the pectoralis muscles, possibly making the patient feel compromised.
There are two methods that I know of:
Rotate and lateral flex the head to the opposite side you are evaluating. This brings the rib head (costotransverse and facet) closer to the surface. But it causes the trapezius, levator scapulae, and scalenus anticus muscles to become taut.
Rotate and lateral flex the head toward the side you are evaluating. This causes the rib to go slightly from the surface. However, as the head is rotated and lateral flexed the musculature creates a "pocket," an invagination, an indentation.
I prefer the later simply because when you follow the pocket in with your thumb as it is being formed by rotating and lateral flexing the head, you will be "directed" to the first rib. Challenge the first rib with a light springing of the articulation. If the problem is the first rib, it will be very, very tender to the patient.
Caution
I will have to assume here that when you challenge the rib that your contact is NOT on the carotid artery and/or any portion of the brachial plexus.
Now That I Can Find It, What Do I Do with It?
Move it, of course! I have found that the first rib needs to be "re-seated" into the facet and "re-introduced" to the anterior portion of the transverse process.
Whatever technique you choose to adjust the first rib, make sure you recheck to confirm or deny your adjustment. A word of descriptive research here: If the first rib has been subluxated for any length of time, it will be very, very tender.
Summary
Be aware of the possibility of a first rib subluxation in patients with headaches, shoulder pain, carpal tunnel syndrome, chest pain, neck pain, rhomboid pain, upper and middle thoracic pain, elbow, wrist, and hand pain, etc.
I hope that the above has helped you in your first rib -- specific adjusting. Write me to let me know if I am right in my clinical approach.
Charles Rollis, BS, DC 826 N. Winchester Blvd. Suite 2-D San Jose, CA 95128 Fax: (408) 246-4299
While there may be no “magic bullet” when it comes to health, this should not dissuade patients or practitioners from seeking out ingredients that offer multiple health benefits. When it comes to dietary supplements, there are thousands upon thousands of choices. So, why not choose one that can address pain and assist with mental health? A supplement that can address inflammation, while also preventing certain types of cancer.
This article focuses on nine severe injuries that are generally not diagnosable until the third to fourth week following the date of injury, including how to diagnose these severe injuries. The discovery of any of these injuries early can make a significant difference in the case outcome.
While canes, braces and posts represent extrinsic methods for lessening adductor moment arms, an intrinsic method for lessening the development of medial knee osteoarthritis occurs when the hip abductor musculature and the iliotibial band are strong enough to create a compressive force capable of stabilizing the lateral knee.