The shoulder has the greatest range of motion of any joint in the body. What is often overlooked in shoulder mechanics is that motion in the shoulder is not purely at the glenohumeral joint. The significant range of motion of the shoulder is made possible by the coordinated movement at the glenohumeral joint and the scapulocostal articulation.
Identifying proper and dysfunctional movement patterns in various joints can be a great help in understanding the nature of certain pathologies affecting those joints.
The Scapulohumeral Rhythm
The scapulocostal articulation is where the scapula articulates with the posterior rib cage. It isn't a true synovial joint, but is considered an articular contact point where bones meet (scapula and ribs).
The scapula and humerus move in a coordinated pattern for all the primary movements of the shoulder. However, their combined motions are particularly important during shoulder abduction, when they are both moving at near-maximum range capability.
Understanding how movement at the glenohumeral joint and scapulocostal articulation occur together is critical for awareness of the dysfunctional mechanics that occur in certain shoulder problems.
Maximum abduction of the shoulder is considered to be about 180 degrees. Note that all the following descriptions about range of motion will be based on the assumption of 180 degrees of abduction. When the shoulder is abducted, motion is occurring at both the glenohumeral joint and the scapulocostal articulation. The combination of movement between the glenohumeral joint and the movement at the scapulocostal articulation is referred to as the scapulohumeral rhythm (also called the scapulothoracic rhythm).
The purpose of this combined movement is twofold. First, it allows the glenoid fossa to maintain a good position for the various roll, spin and glide movements of the humeral head at the glenohumeral articulation. Second, the changing position of the glenoid fossa allows for a better length-tension relationship in the muscles acting across the glenohumeral joint to produce shoulder motions.
Two Elements: Abduction, Rotation
There are two primary components of the scapulohumeral rhythm. The first is abduction of the glenohumeral joint, which is produced primarily by the supraspinatus and the deltoid muscles. The second part of the scapulohumeral rhythm is upward rotation of the scapula, and is produced primarily by the upper and lower fibers of the trapezius, as well as the serratus anterior muscle.
If the scapulohumeral rhythm is properly coordinated, an individual will have approximately 120 degrees of glenohumeral abduction and 600 of scapular upward rotation. Therefore there is roughly a 2:1 ratio of movement in the glenohumeral joint to that of the scapulocostal articulation.
It is important to note that these motions are not sequential, but almost concurrent. That means most of the glenohumeral abduction and the scapular upward rotation will be occurring at the same time.
A common misunderstanding about glenohumeral abduction relates to supraspinatus activity during abduction. Many texts report that the supraspinatus muscle initiates abduction and is active for the first 25-40 degrees of abduction. It is then sometimes suggested that the deltoid takes over to perform the remainder of the abduction movement without further supraspinatus involvement, which is not accurate.
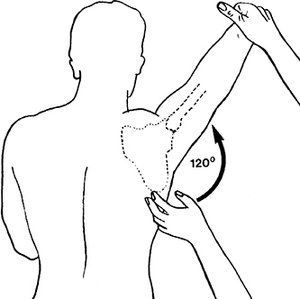
Figure 1
The supraspinatus muscle remains active throughout the entire movement of abduction. It is most active during the early stages when there is very little deltoid activity, but it does not stop its contraction process throughout the entire abduction movement.
Figure 1 shows the humerus at 120 degrees of abduction. Some of the motion has occurred at the glenohumeral joint and some at the scapulothoracic articulation. So, using the idea of our 2:1 ratio, there has been about 80 degrees of abduction at the glenohumeral joint and about 40 degrees of upward rotation of the scapula: 120 degrees of abduction.
Long Thoracic Nerve Entrapment
Understanding how these movements at the glenohumeral and the scapulocostal articulations work together is extremely important when looking at certain shoulder complaints. When there is a disturbance to the scapulohumeral rhythm, it can play a significant role in shoulder pathologies. As an example of how the scapulohumeral rhythm plays a part in shoulder pathologies, let's take a look at what happens with eventual results of long thoracic nerve entrapment.
The long thoracic nerve innervates the serratus anterior muscle. This nerve exits the spine very close to the brachial plexus and is often involved in brachial plexus injuries. It can also be injured when people wear heavy backpacks or anything with heavy shoulder straps.
An injury to the long thoracic nerve may impair function in the serratus anterior muscle, causing it to be weak. Serratus anterior weakness from long thoracic nerve compression is often evident with patients who display a winging scapula.
When the serratus anterior is not working properly, it doesn't pull the scapula into upward rotation far enough during abduction movements, and the humerus may hit the underside of the acromion process near the end of the abduction movement, causing shoulder impingement and potential rotator-cuff pathology.
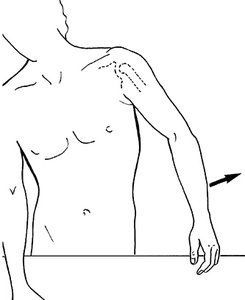
Figure 2
Adhesive Capsulitis (Frozen Shoulder)
Another common example of the importance of the scapulohumeral rhythm is illustrated with dysfunctional movement patterns that occur when a patient has adhesive capsulitis of the shoulder (also called frozen shoulder). With this condition, the glenohumeral joint capsule will adhere to itself and not allow full glenohumeral abduction. When this occurs, there will be a very evident disturbance in the scapulohumeral rhythm.
Any attempts at abduction in this scenario will usually require significant substitution, so you will often see a motion like that pictured in Figure 2. There is a significant bind to glenohumeral abduction, and the patient is trying to compensate with additional upward scapular rotation and lateral flexion of the torso.
In order to understand the best way to treat various shoulder problems, we must be able to recognize and evaluate both correct and dysfunctional movement patterns. Appreciating the scapulohumeral rhythm is a big step in the right direction.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.