Hip Flexor Contractures & LBP in Above-the-Knee Amputations
William E. Morgan, DC;
Clare P. Morgan, DC
Patients with above-the-knee amputations (AK or AKA) are particularly prone to developing hip flexor contractures. Not to be confused with muscle tightness, contractures are a permanent shortening of tissues which cause deformity or distortion. They also can lead to pelvic and spinal complications, including back pain, anterior pelvic tilt and lumbar hyperlordosis when a patient begins walking with a prosthetic limb. In fact, 81 percent of patients with a transfemoral amputation will experience lower back pain, with severe back pain reported by more than 25 percent of those with amputations.
Three Causes of Hip Flexion Contractures Following Above-the-Knee Amputations
Following an amputation, particularly a traumatic amputation, the main concern by the medical team may not be the effect on the patient's future gait, biomechanics or spinal mechanics. They are concerned with patient survival, wound healing, infection and thromboembolism. As healing progresses, inpatient rehabilitation will address hip flexion contractures, of which there are three main causes:
Sitting in a wheelchair while waiting for the residual limb (stump) to heal allows the amputation to heal in a flexed posture. (Figure 1)
The insertions of the strong hip flexor muscles (psoas and iliacus) remain wholly intact in an AKA, while most of the insertions of their antagonist muscles are amputated. The antagonist insertions of the semitendinosus, semimembranous, biceps femoris and iliotibial band (which is essentially the tendon of the gluteus maximus) are gone, while the powerful hip flexor muscles remain intact. Thus, the counterbalance of strong hip extension is greatly diminished. The shorter the residuum, the greater the likelihood of contracture.
The Effects of Hip Flexion Contractures in AKA
Hip flexor contractures create a problem when AKA patients transition from using a wheelchair to using prosthetic limbs. If an uncompensated prosthetic socket is used, the hip flexors will create a hyperlordosis of the lumbar spine when the patient begins to walk upright. (Figure 2) This also may create asymmetrical torsion of the lumbopelvic region in cases with unilateral AKA. These aberrant patterns can cause lumbar facet and sacroiliac dysfunction.
Contractures, even if accommodated by a specially fashioned prosthetic socket (Figure 3), will limit the stride length of that limb.
Identifying Shortened Hip Flexors
Contractures and muscle tautness are not the same. Contractures can be permanent or near permanent. Contractures occur when connective tissue loses its normal elasticity and flexibility. The tissues become shortened, stiff, inflexible and infiltrated with tough, fibrous tissue.
In many patients with AKA, hip flexor shortening can be identified by simply having the patient lie supine. If the residual limb points up instead of lying flat, it is a sign of hip flexor shortening.
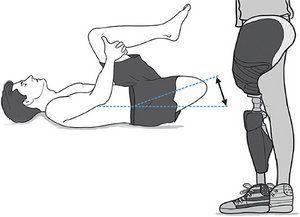
Another method to determine hip flexor shortening is the Thomas test (Figure 4), performed with the patient lying supine on an examination table. The patient or doctor flexes the patient's leg toward the chest until the thigh contacts the abdomen or the lumbar lordosis is flattened. If the non-flexed thigh remains on the examination table, the Thomas test is negative. If, however, the leg rises from the table, it is indicative of tightness in the hip flexors. To establish a baseline metric, measure the amount of tightness with a goniometer.
Caring for patients with amputations, especially recent amputations, should involve a team. This team usually includes physiatrists, prosthetists, physical therapists, orthopedic surgeons – and increasingly, chiropractors.
Spinal problems arising from AKAs can and should be treated with chiropractic adjustments, utilizing techniques intended to normalize the sacroiliac joints, facets and other spinal structures. The underlying problems of hip extensor weakness and hip flexor contractures also must be addressed in a rehabilitation program.
If performing side-posture adjustments, I recommend having the patient leave the prosthetic limb on. This will provide a lever arm to give you, the chiropractor, a mechanical advantage. However, in cases of high transfemoral amputation, the prosthetic limb may fall off during treatment. If this occurs, move the limb aside and perform the adjustment without the prosthetic leg.
To make the patient more comfortable, I usually use a folded towel as a pad between the metal shaft of the prosthetic limb and the bones of the knee or tibia when performing a side-posture adjustment.
While chiropractors strive for symmetry and balance, it is difficult or even impossible to attain symmetry in treating amputees. In reality, the patient will adapt to a new functional normal, which will likely have asymmetry. This adaptive asymmetry is part of the body's ability to compensate and adjust to impairment.
One thing that should be avoided is the use of traditional leg-length indicators to determine how to adjust the patient. These methods are less consistent in this population of patients.
If, through the course of treatment, the patient's hip flexion contracture is diminished and hip extension strength is normalized, then re-evaluation should be done by the patient's prosthetist, who may revise the socket's angle.
Treating amputees with hip flexor contractures requires an understanding of the condition and the options available. Preventing contractures in the early stages of healing is certainly much easier than trying to correct or compensate for them later.
Disclaimer: The views expressed in this article are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of the Army, Department of Defense or the U.S. government.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.