As you know, posture reveals a great deal about the body. Posture is a unique mental and physical landscape revealing compensations and adaptations to life. It's a classic mind-and-body story. As clinicians, we must be open and attune to hearing and seeing the story. Observing, listening, touching and moving are fundamental steps of discovering the underlying truth. The clinical audit process guides us in the journey.
Compensation, dysfunction and pain are requests for change. The brain and body are communicating their need for something different. We simply need to listen.
A common posture story is an elevated shoulder/scapula. Let's take a look at one culprit in detail, including how to identify the problem and then address it.
Quadratus Lumborum Inhibition
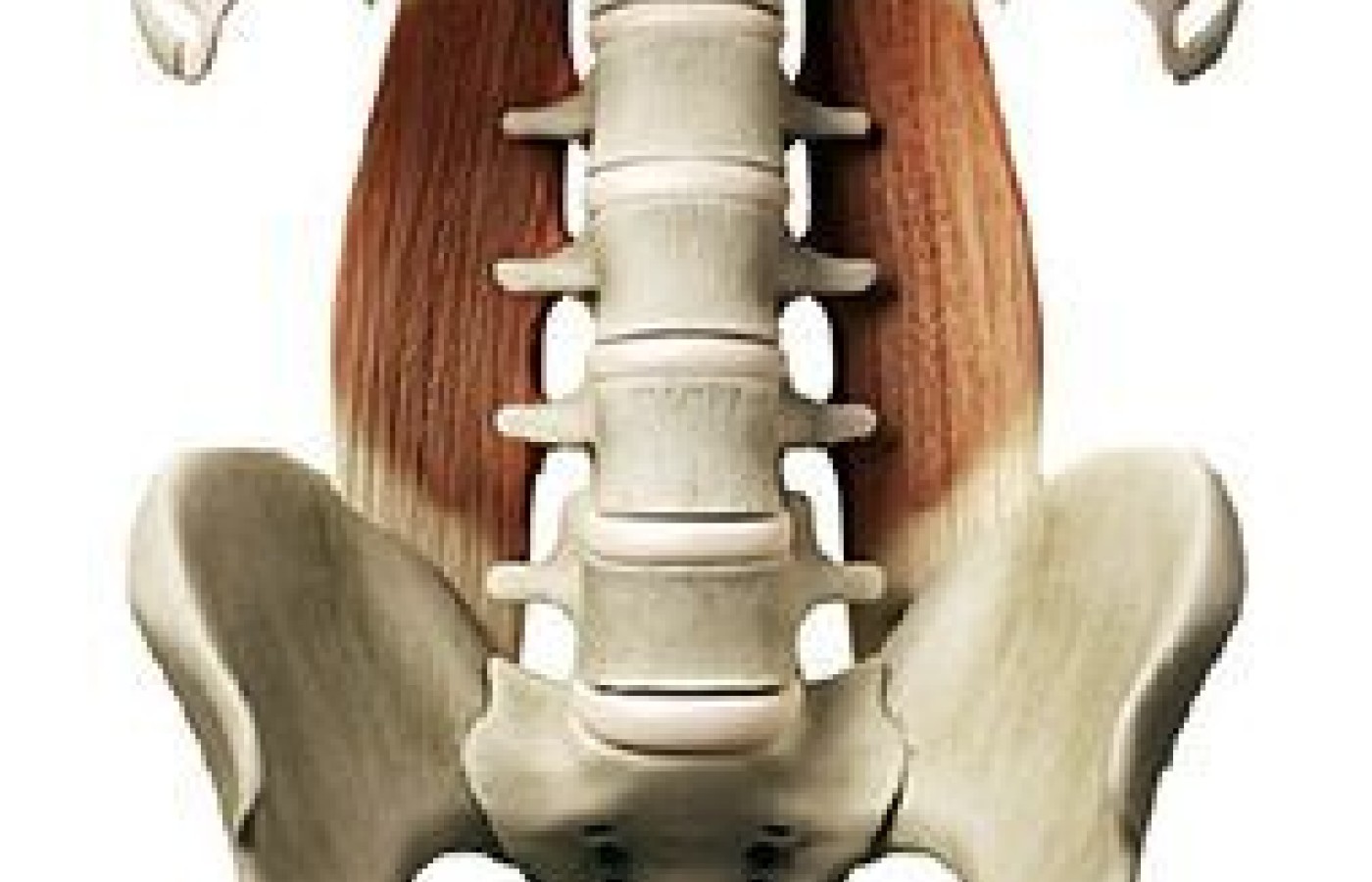
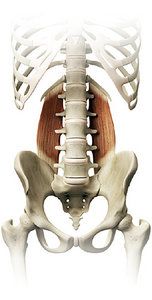
The quadratus lumborum (QL) originates on the posterior iliac crest and inserts on the last rib and transverse processes of the first through the fourth lumbar vertebrae. It's action is to unilaterally tilt (elevate) the pelvis, laterally flex the vertebral column to the same side and assist in extending the vertebral column.
If the quadratus lumborum becomes inhibited, the pelvis drops on the ipsilateral side and the lateral subsystem (LSS) of movement stabilization will become dysfunctional (quadratus lumborum, contralateral hip adductors and abductors). When this occurs, the opposite-side quadratus lumborum may become neurologically unregulated and facilitated, causing lateral flexion of the torso.
Lack of central zone stabilization of the LSS during bipedal locomotion causes a compensatory elevation of the shoulder on the side of the inhibited quadratus lumborum. What looks like an elevated shoulder is actually a dropped pelvis from an inhibited QL.
Assessment
Evaluate the quadratus lumborum for hyper/hypotonicity. Palpate and compare bilaterally. Suspect inhibition when you discover hypotonicity.
Have the patient perform a side plank for 20 seconds on one side and then 20 seconds on the other side. Compare strength of the plank by side. The weaker side must be assessed further for inhibition. If there is pain during the assessment, you already know there is dysfunction in the pattern. Also note if the downside shoulder is elevating toward the head during the plank.
With the patient in a standing position with their feet together, instruct them to raise both arms overhead. Observe spacing between the pelvis and rib cage on each side. The inhibited side will have more space. Now have the patient laterally flex to the right and the left with their arms overhead. Observe how far they get and their overall movement efficiency. The side with less motion may indicate inhibition (not strong enough to get you there) and facilitation on the opposite side (too tight to let you get there).
Muscle test the quadratus lumborum on both sides to compare neurological engagement and strength. Patient is supine on table. Move straight legs 6 inches to the left, away from midline. Stand on the right side of the patient, facing table. Place left hand on the outside of the right hip and right forearm underneath both ankles, grabbing the left ankle. Pull legs back toward center while stabilizing the right hip as patient resists your pressure. You are testing the left quadratus lumborum.
Now move the legs 6 inches to the right away from midline. Stand on the left side facing table. Place your right hand on the outside of the left hip and left forearm underneath the patient's ankles, with the left hand grabbing their right ankle. Pull legs back to the center and have them meet your pressure. This is assessing the right quadratus lumborum.
Inability to hold and resist the muscle test is a sign of inhibition. Now go back and retest the first QL side again (in this example, the left) to see if it changes. Why? You are checking a pattern. By going back, you are observing how muscles react to each in a pattern. Both sides should be strong. If either QL goes weak, it indicates dysfunction.
Interventions
The goal here is to establish a pattern of function in a stable environment. Soft-tissue therapy bilaterally to the QL muscles will help release tension and fascial restrictions. Also release the tissue surrounding the opposite-side anterior-superior iliac spine (ASIS). The contralateral anterior hip and thigh region become overworked when the quadratus lumborum is inhibited and the pelvis drops. Tenderness is most often felt on the medial border of the ASIS.
Have the patient perform an ipsilateral crawling pattern on the ground on the inhibited side. The ipsilateral crawl integrates full-body patterning with a low-load threshold stabilization strategy. Then progress them to a supine, single-leg-stance, isometric-hold movement.
Example with left QL inhibition: Instruct patient tolie on the ground in a prone position with their arms overhead and legs straight. Patient turns their head to the left and then brings the left knee and left elbow together in a crawling pattern, holds for 4 seconds and returns. Repeat four times.
Next, instruct patient to lie supine with arms overhead and legs straight. Patient brings right leg into hip-flexion, single-leg-stance position and holds for 4 seconds; then lowers back to the ground and repeats four times. Make sure knee passes the waist midline.
Ida Rolf once said, 'Where you think it is, it ain't.' That should be a mainstay of musculoskeletal pain assessment. Start where it hurts and then look elsewhere. Observe posture and movement, look for the pattern of dysfunction and you will find the answer.
Pain only tells you there is a problem, it does not tell you what it is. Full-body assessment is a linchpin to unlocking the posture and movement story.
Resources
Biel A, Dorn R. Trail Guide to the Body: A Hands-on Guide to Locating Muscles, Bones, and More. Boulder, CO: Books of Discovery, 2010.
Cook G. Movement: Functional Movement Systems: Screening, Assessment, & Corrective Strategies. Aptos, CA: On Target Publications, 2010.
Bond M. The New Rules of Posture: How to Sit, Stand, and Move in the Modern World. Rochester, VT: Healing Arts, 2007.
Weinstock D. NeuroKinetic Therapy: An Innovative Approach to Manual Muscle Testing. Berkeley, CA: North Atlantic Books, 2010.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.