How to Assess Patients' Footwear for Postural Conditions
Mark Charrette, DC
A shoe is like a book: If you know how to read one, you can learn a great deal. If you "read" your patients' shoes, you can discover much about their postural conditions. Worn-out shoes and shoes that don't fit properly can interfere with the feet, pelvis and spine. For example, a survey on women's shoes found 88 percent of the women surveyed were wearing shoes smaller than their feet (average 12 cm smaller)1. Is it any wonder 80 percent of the women in the study reported "some foot pain" and 76 percent had one or more forefoot deformity?
Fit Is Critical
Putting your foot into a shoe is like putting it into a cast. Poor-fitting, unsupportive shoes can cause problems. When assuming the weight-bearing posture, the patient should be able to palpate the large toe joint and find it positioned at the widest part of the shoe. If the joint is forward of this area, the shoe is too short (you'll seldom find the shoe is too long).
As a general rule, when a shoe is ill-fitting, it is usually short and wide. Shoes that are broken down, vamps pushed over (the top of the shoe pushed laterally), with uneven heel and sole wear usually tell a story. Here's how to interpret it.
Heel Wear
Normal heel wear is slightly lateral of the midline. Heel wear should be even on both sides. If one side is worn more than another, this can indicate a weakness on that side.
Usually in my practice, I find the shoe that has the most wear is on the same side as my patient's knee, hip, or spinal problem. Observe the heel wear – you'll be amazed.
Sole Wear
Turn the shoe over and examine the sole wear. Start at the toe and let your eyes follow the sole wear toward the heel. At the point at which the sole wear "feathers out" and stops, draw a horizontal line with a pen or pencil. Repeat the same procedure with the opposite shoe. Determine which shoe demonstrates sole wear closest to the heel. If you find visualization difficult, measure with a ruler.
When one shoe has more sole wear than the other, usually the foot pronates more – causing faster shoe breakdown and sole wear.
The shoe that demonstrates the sole wear beginning closest to the heel indicates the side of greatest pronation. Further examination will reveal the patient usually has a weak psoas, weak abductors, and weak neck flexors on that side (unless trauma is a factor). The patient may have symptoms including one or more of the following: knee pain, hip pain, lumbosacral or sacroiliac involvement, or cervical problems on that side (again, unless trauma is a factor). If the shank is breaking down excessively, recommend the patient purchase new shoes.
Proper footwear will do much to help your adjustments hold better. Restoring balance to the pedal foundation can be accomplished far more effectively if you take a few moments to instruct the patient as to the type of shoe that will be best for their particular condition. Generally speaking, a good lace-type shoe with firm counter is best.
What to Tell Your Patients
Make sure shoes fit properly; the ball of the foot should be positioned at the widest point of the shoe.
Remove any generic insoles from shoes before inserting orthotics.
Old, broken-down shoes should be thrown away immediately and replaced with new shoes.
Buy shoes like you would fruit: squeeze them in the heel area. You want a firm counter around the heel to help support pronated feet. (Supinated feet need a "squishy" or soft counter.)
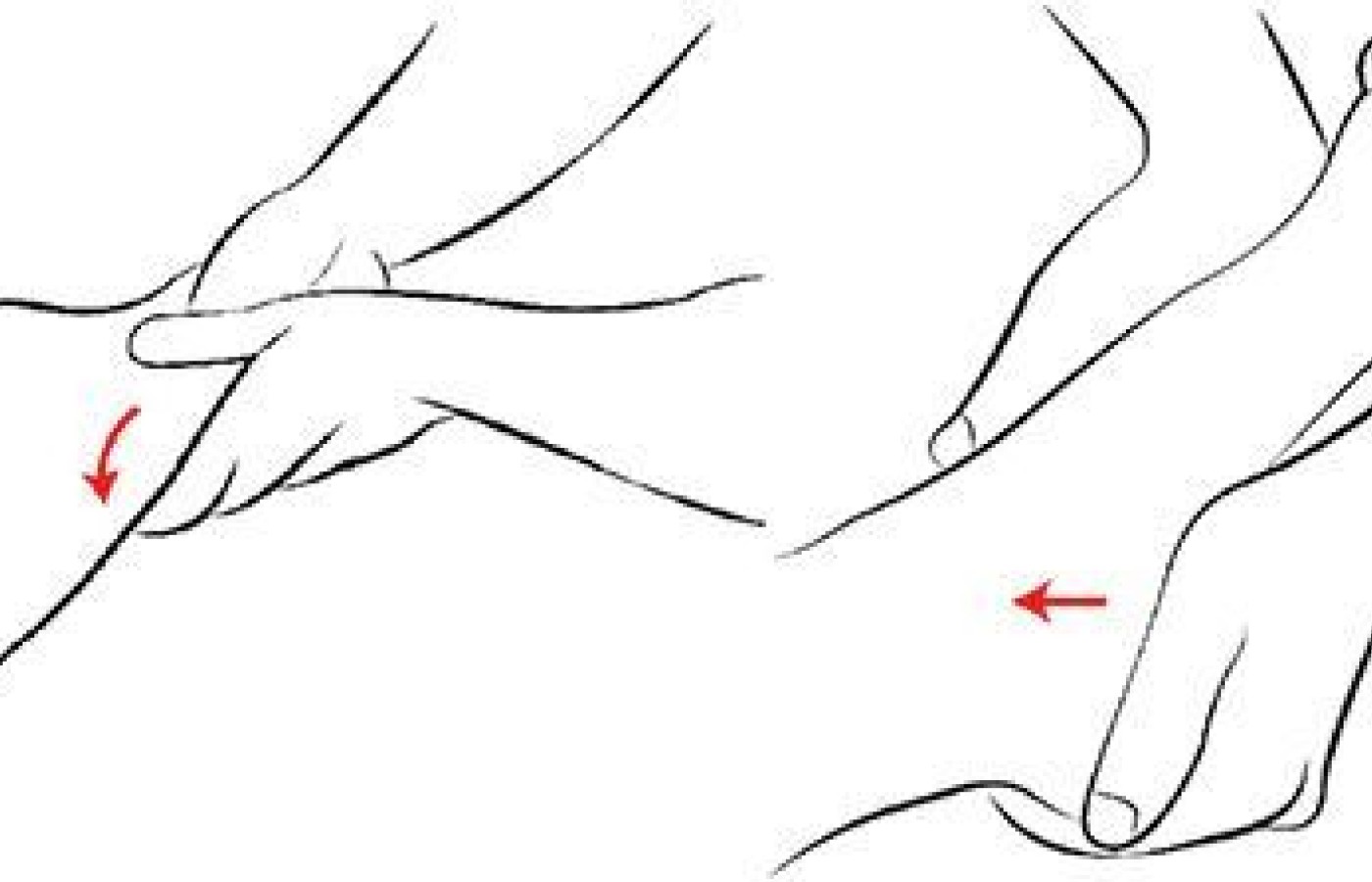
Fig. 1A/B The navicular adjustment.
Extremity Adjusting: Navicular
There will be point tenderness in an area on the longitudinal arch (plantar surface) anterior and medial to the calcaneus. (Fig. 1a) The psoas also will become weak with this misalignment.
Contact the area of point tenderness with the thenar of the thrusting hand while the other hand stabilizes along the lateral aspect of the foot. Then bring the foot to tension in a medial direction. Thrust is toward the lateral malleolus, which is superior and lateral (Fig. 1b). The psoas muscle test (Fig. 2) can be used to demonstrate to doctor and patient the effectiveness of a navicular adjustment. Pre-adjustment, the psoas is "weak," while post-adjustment, it is "strong."
Fig. 2 The psoas function test.
Once you have found the appropriate adjustment for your patient, orthotics can help hold the navicular adjustment in place.
Your patients' feet may feel just fine, but that doesn't mean they're not causing trouble up above. Foot imbalance or dysfunction can have ripple effects, transferring problems (and pain) to the legs, knees, hips, spine, shoulders and even skull. Assessing patients' feet and their footwear can help you detect these "silent" problems, leading to a better, more holistic understanding of their health issues and how to approach them.
Reference
Frey C, Thompson F, et al. American orthopaedic foot and ankle society women's shoe survey. Foot & Ankle, 1993;14:78-81.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.