Pain in Motion: Neck Pain Caused by Sternocleidomastoid Imbalance
Perry Nickelston, DC, FMS, SFMA
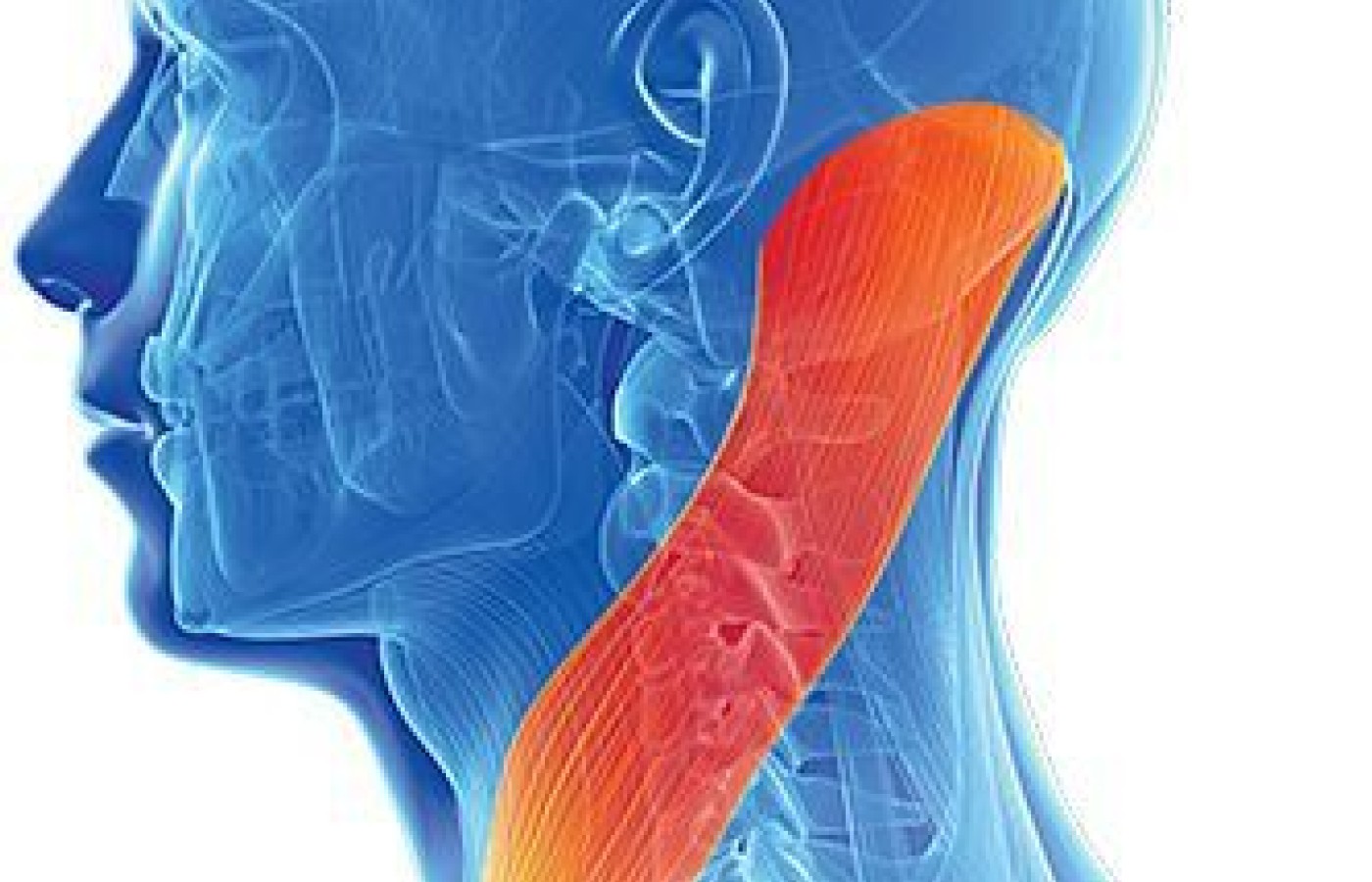
The sternocleidomastoid muscle (SCM) can be an elusive contributor to neck pain because of its critical role in stabilization and equilibrium. The SCM is one of the most complex muscles in the body because of its wide array of muscle-patterning actions and intricate connection to force transmission via the fascial lines. It functions as both a short-range (clavicular head) and long-range (sternal head) rotator, an upper cervical extensor, a flexor of the cervical spine, a lateral flexor, as well as a source of equilibrium sense.
When the SCM becomes dysfunctional as a result of myofascial trigger points (TPs), whiplash-type injury, impact trauma in sports, or poor sleeping habits, it can wreak havoc on the movement system of the body. An imbalance in SCM patterning with either inhibition (neural down-regulation) or facilitation (neural up-regulation) may cause compensatory reactions from other areas of the body far removed from the neck. In movement patterning, the head rules the movement road. The body follows where the head goes.
Just observe a baby looking around and exploring the world trying to learn. The baby sees a toy, turns their head toward the toy, reaches for the toy and tries to move the entire body toward it. Try reaching for something without looking at it; not an easy task.
Righting Reactions and Patterns of Compensation
When we grow and begin to move on two feet, the inevitable effects of gravity and trauma of daily living take their toll on the body. The neck begins a long journey of compensation to maintain primal righting reactions (RR). Righting reactions develop at or shortly after birth in response to gravity. They are most distinguishable at 10-12 months of age and remain active throughout life, providing integrated movement between the head and torso. They are critical to our relationship with gravity and between body segments, and allow us to orient our body to the environment. There are two general categories of RR:
Bringing the head into upright or vertical orientation in space in relation to gravity
Bringing the head and trunk into mutual alignment with each other
RR underlie movement transitions and are required for standing, walking, running, etc., and maintaining postural alignment / tone. They are intrinsic automatic reactions to a rapid loss of balance and weight shifting. What happens when a component of the RR, such as the SCM, is compromised? Compensation. Imbalance in the RR may lead to cervical fixation for stability.
The brain will choose a local or global compensation for a dysfunctional SCM pattern. The body is interconnected. There is no break in living matter. For example, if there is inhibition of the right SCM, a local synergistic muscle in the neck, such as the scalenes, may take over the extra force production necessary for movement. As a result, the scalenes become overworked and painful.
Let's take the same right SCM and search for a possible global compensation. The lateral (frontal-plane) line of the body includes the side of the neck, upper extremity, torso and lower extremity. If lateral flexion of the neck is compromised from an inhibited SCM, force transmission may be compensated for in the quadratus lumborum.
Think of standing with your feet together and then taking a side step to the right. Can you see and feel how the entire right side forms a pattern of movement? Thus, a patient having right-sided QL pain may have a link to neck dysfunction.
Evaluate the SCM for trigger points, muscle tone (hypertonicity / hypotonicity) and activation. Perform a range-of-motion assessment and note restrictions, pain or discomfort. Also perform a supine isometric hold assessment for muscle activation: Patient lies on their back; flex the head forward and rotate to one side, holding for 10 seconds. Repeat bilaterally. Note difficulty on performing the isometric hold, pain, discomfort and/or compensations. The side with greater difficulty indicates inhibition.
A Clinical Example
A patient complains of chronic right-sided neck pain. Hypotonicity and inhibition of the left SCM and weakness of right cervical rotation with isometric hold. Increased pain in the right side of neck with rotation. Fixation of lower cervical spine at C6-C7.
Release the right cervical musculature, adjust cervical fixation, and retest the right rotation to activate the inhibited left SCM.
When pain is on board, muscle patterning should be evaluated. Think beyond individual muscles when treating musculoskeletal pain. The brain takes the path of least resistance for movement patterning. If there is difficulty in moving the neck efficiently, the brain will simply choose another path of less effort. When assessing any musculoskeletal pain syndrome, the neck should always be considered a player, particularly the sternocleidomastoid.
Resources
Benzel EC, Clark CR. The Cervical Spine. Philadelphia: Lippincott Williams & Wilkins, 2005.
Berger D. "Primitive Reflexes and Righting Reactions: A Look Through the Lense of Survival, Emotions and Memory." (Work in progress)
Peterson BW, Richmond EJ. Control of Head Movement. Oxford University Press, New York, 1988.
Weinstock D. NeuroKinetic Therapy: An Innovative Approach to Manual Muscle Testing. Berkeley, CA: North Atlantic, 2010
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.