Posterior ankle impingement syndrome, PAIS, is a term used to describe a musculoskeletal disorder created from the repeated abutment of the posterior process of the talus or os trigonum between the tibia and calcaneus during plantarflexion of the ankle. The repetitive plantarflexion of the foot causes compression and entrapment of soft tissues, bony processes or unfused ossicles between the posterior-tibial plafond and the superior surface of the calcaneus; similar to nuts in a nutcracker. As a result, bone contusions and local synovitis develop in the tibiotalar and subtalar joints.1
The normal anatomical variations that predispose one to PAIS include the following: down-slope of the posterior tibia; an os trigonum; a prominent posterior talar process (Stieda process);1 prominent tuberosity arising from the superior calcaneus; and presence of the posterior-intermalleolar ligament (PIML).2 In addition to these anatomical variations, generalized hypermobility or previous disruption to the anterior talofibular ligament and subsequent anterior talocrural laxity may predispose some to PAIS.
Figure 2: Foot X-ray showing extreme plantarflexion in a ballet dancer while en pointe.
When the os trigonum is the cause, it is described as os trigonum syndrome. Os trigonum is caused by the failure of fusion of the secondary ossification center which forms the posterolateral aspect of the talus. This secondary ossification center develops between the ages of 8 and 13 years. Normally this ossification center fuses with the rest of the talus within one year. If it fails to fuse, an os trigonum is formed that articulates with the talus via a synchondrosis.1,3-4 (This is a good reason to recommend that young female ballet dancers not be put en pointe before 14 or 15 years old.)
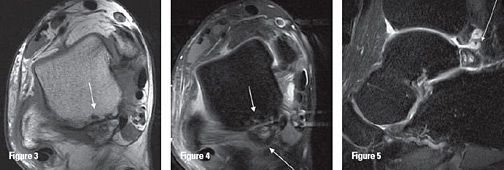
Figures 3-5 (left to right): Axial PAIS T1, Axial PAIS T2 and Sagittal PAIS T2. Patchy areas of altered marrow signal, appearing hypointense on axial T1-weighted image and hyperintense on the axial T2-weighted image, suggest bone marrow edema. Subchondral erosions are seen along the articular margins (small arrows). Ill-defined hyperintense signal in the soft tissue around the os trigonum (long white arrow).
PAIS in the presence of an os trigonum may be associated with additional irritation of the synchondrosis, causing the development of secondary inflammatory tissue that may perpetuate the cycle of impingement and inflammation. PAIS is common in ballet dancers, but is also encountered in those who participate in other sports that involve forced plantarflexion of the foot, such as soccer, basketball, and volleyball.1
Typically, patients describe pain localized to the posterior aspect of the ankle, which is aggravated by forced plantarflexion activities; e.g., dancing en pointe position (ballet), kicking, downhill running, the take-off phase of horizontal jumping, walking (basketball, volleyball) and even wearing high-heeled shoes. Upon examination, there generally is tenderness on palpation in the region of the posterior ankle joint and the most posterior aspect of the subtalar joint. The reproduction of pain on forceful plantarflexion, and sometimes on resistive plantarflexion or dorsiflexion of the big toe, are considered hallmarks of PAIS.
The differential for posterior ankle pain can be daunting, but often the history / clinical presentation is pathognomonic, especially in athletes. Other causes of posterior ankle pain include:
Achilles tendon pathology
Retrocalcaneal bursitis
Sever's disease in adolescents
Accessory soleus muscle
Referred pain from lumbar spine
Peroneal tendon subluxation
Ankle osteoarthritis
Tarsal tunnel syndrome
Haglund's deformity
Tarsal coalition
Inflammatory arthropathies
Calcaneal stress fracture
Tibialis posterior tendinopathy
Flexor hallucis longus (FHL) tendinopathy
Medial calcaneal nerve entrapment
Radiographs can be helpful revealing an os trigonum or Stieda process. Lateral radiographs obtained with the foot in plantarflexion may demonstrate the os trigonum or lateral talar tubercle impinged between the posterior-tibial malleolus and the calcaneal tuberosity.1 MR imaging is the modality of choice for further evaluation of the bony and soft-tissue structures.
MRI of the ankle can demonstrate bone marrow edema within the os trigonum and at synchondrosis with the posterior talar tubercle, which is considered a reliable sign of PAIS.1,5 Other common sites of edema include the posterior talus and the posterior calcaneus. MRI can demonstrate fractures, if present, through the os trigonum that are difficult to evaluate with plain films.
The additional inflammatory changes in the adjacent soft tissues can also be demonstrated on MRI, including edema or enhancement of posterior soft tissue, indicating posterior tibiotalar joint synovitis caused by the repetitive compression and posterior-capsular thickening. There can be fluid around the flexor hallucis longus (FHL) tendon or synovial enhancement, which is caused by tenosynovitis of the FHL and high signal changes and/or enhancement within the musculotendinous junction of FHL muscle belly due to impingement.5-6
Most patients will respond to conservative treatment that includes anti-inflammatory agents, activity modification, weight-bearing immobilization, and physiotherapy. If conservative measures fail, open or arthroscopic surgical excision of the abnormal accessory bone may be recommended.
References
Bureau NJ, Cardinal E, Hobden R, Aubin B. Posterior ankle impingement syndrome: MR imaging findings in seven patients. Radiology, 2000;215:497-503.
Rosenberg ZS, Cheung YY, Beltran J, et al. Posterior intermalleolar ligament of the ankle: Normal anatomy and MR imaging features. Am J Roentgenol, 1995;165:387-390.
Robinson P, White LM. Soft-tissue and osseous impingement syndrome of the ankle: role of imaging in diagnosis and management. Radiographics, 2002;22:1457-1469.
Karasick D, Schweitzer ME. The os trigonum syndrome: imaging features. Am J Roentgenol, 1996;166:125-129.
Hamilton WG, Geppert MJ, Thompson FM. Pain in the posterior aspect of the ankle in dancers. Differential diagnosis and operative treatment. J Bone Joint Surg (U.S.), 1996;78:1491-1500.
Peace KA, Hillier JC, Hulme A, Healy JC. MRI features of posterior ankle impingement syndrome in ballet dancers: a review of 25 cases. Clin Radiology, 2004;59:1025-1033.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.