Rheumatoid arthritis (RA) is one of the most common inflammatory arthritides encountered. The condition is most often seen in women 20-50 years of age.1 RA occurs as a result of an autoimmune response to an antigen present on the synovial membrane, causing an inflammatory reaction.1 It affects synovium-lined joints, bursae and tendon sheaths, cartilaginous joints, and sites of ligament and tendon attachments to bone.2 This reaction results in a proliferation of the synovium called pannus. This reaction sets in motion the sequence of joint destruction in RA. The posterior joints of the cervical spine can be involved, and in the appendicular skeleton, its pattern is characterized by a bilateral, symmetric distribution.2
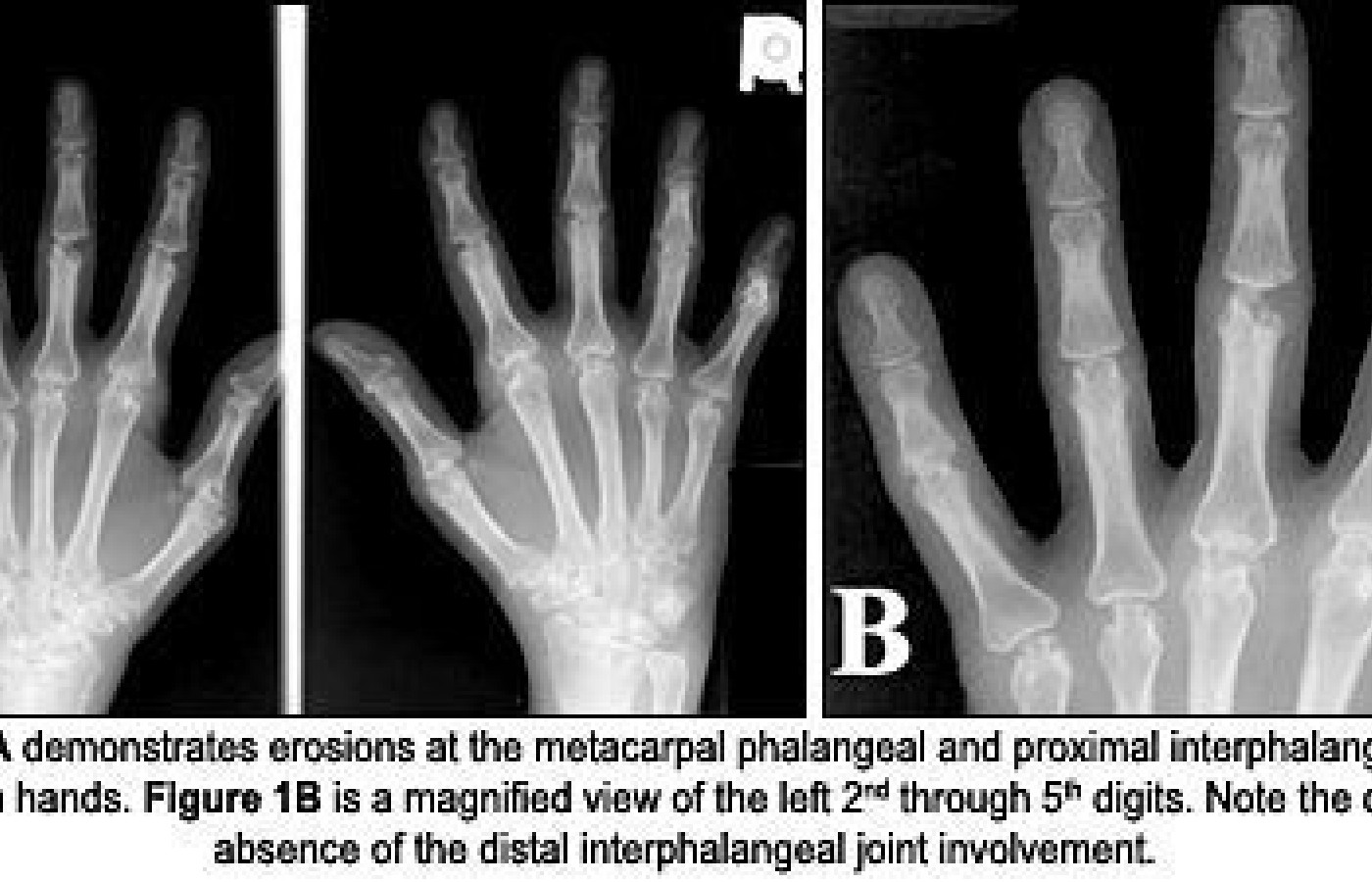
Radiographic findings for rheumatoid arthritis occur in stages. Early on, the initial finding will be soft-tissue swelling around the affected joint. As the condition progresses, there will be periarticular osteoporosis due to the hyperemia at the joint, followed by loss of joint space and bone erosion, due to pannus destruction of cartilage and unprotected bone. Erosions will occur at the outer margins of the joint, where there is no protective hyaline cartilage - commonly referred to as the "bare area" of the joint. As progress of the disease continues to the later stages, there will be diffuse osteoporosis, due to corticosteroid therapy and disuse, as well as joint malalignment from ligament and muscle laxity. In the hands, the pattern of involvement consists of metacarpophalangeal (MCP), proximal interphalangeal (PIP) and carpal joint involvement. There is distinct absence of distal interphalangeal (DIP) joint involvement of the hands with RA. (See figures 1A and 1B.)
In the spine, the severity of RA varies. Up to 80 percent of patients with rheumatoid arthritis will have involvement of the cervical spine.2 The concern for chiropractors is upper cervical instability from pannus-induced erosion at the insertion of the transverse ligament of the atlas, causing disruption or laxity of the ligament. Flexion and extension stress radiographs are necessary to assess the relationship of the anterior tubercle of C1 to the dens. Instability is found if the atlantodental interspace (ADI) exceeds 3 mm in adults or 5 mm in children under the age of 16. The facet or zygapophyseal joints of the cervical spine, while synovial joints, are also affected by RA; however, it is very difficult to visualize joint erosions in the small joints of the spine with plain-film radiographs.
RA also affects some of the soft tissue throughout the body. Up to 20 percent of patients with RA will develop soft-tissue nodules, primarily in the subcutaneous tissues, but these may also occur within organs or bone.2 In addition to developing nodules, approximately 5 percent of RA patients will develop bursitis.1 The most significant potential consequence of the musculoskeletal soft-tissue involvement is tendon ruptures due to pannus proliferation at synovial sheaths. This occurs commonly at the hand and wrist, as well as the supraspinatus tendon of the shoulder, which results in superior migration of the humerus in relation to the glenoid process.
Treatment for RA is variable and dependent upon patient presentation. For the chiropractor, it is important to proceed cautiously when contemplating adjustive treatment, as there may be muscle and/or ligamentous laxity that can lead to instability at any joint involved. It is important enough to repeat that the chiropractor must determine that there is no upper cervical instability with stress views of the cervical spine prior to attempting adjustive techniques in the cervical spine. Referral to a rheumatologist is part of a wise plan; the progression and disabling nature of RA needs to be addressed with all available resources. The more common medications used to treat RA consist of a class of drugs called disease-modifying antirheumatic drugs (DMARDs) The goal of these drugs is to block autoimmune reaction, rapid cell turnover and joint destruction. There are several medications within this class of drugs, and their most significant side-effect is increased susceptibility to infection.
References
Resnick D, Niwayama G. Diagnosis of Bone and Joint Disorders, 3rd ed. Philadelphia: W.B. Saunders 1995.
Yochum T, Rowe L. Essentials of Skeletal Radiology, 3rd edition, Baltimore, Williams & Wilkins 2005.
Marchiori D. Clinical Imaging with Skeletal, Chest and Abdomen Pattern Differentials. Mosby, St Louis, 1999.
Bassano J. Radiologic review of the arthritides. Topics in Clin Chiro 2000;7🔢17-38.
John M. Bassano, DC, DACBR Associate, Professor, Dept. of Diagnostic Imaging Los Angeles College of Chiropractic Southern California University of Health Sciences
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.