The impingement syndrome is a frequently overlooked but important cause of chronic shoulder pain and disability. Impingement occurs when there is encroachment on the subacromial space with loss of the normal sliding mechanism between the superior periarticular soft tissues of the glenohumeral joint and the coracoacromial arch. Entrapment of the soft tissue structures between the coracoacromial arch and greater tuberosity of the proximal humerus during abduction or elevation of the arm results in subacromial bursitis and rotator cuff tendinitis with eventual progression to fibrosis and rupture of the rotator cuff.
Clinically, the impingement syndrome is seen in two main groups of patients. In young athletic patients involved in sporting activities in which frequent and repetitive overhead throwing motions are used (i.e., baseball, football, tennis), the onset of symptomatic impingement frequently occurs before 25 years of age. A second group consists of older patients in whom symptoms may appear spontaneously or in association with sporting activities (golf, tennis) or occupational stresses.
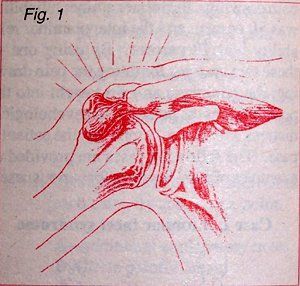
The impingement syndrome is characterized by sharp pain associated with abduction 70-120 degrees, external rotation 20-30 degrees, and internal rotation greater than 30 degrees. Classically, a full range of shoulder motion is present. The severity of the discomfort varies from mildly irritating to totally debilitating. On physical examination, crepitance may be palpated over the superior aspect of the shoulder at the point of impingement. Radiographic evaluation will demonstrate the presence of bony excrescences arising from the anteroinferior aspect of the acromion (subacromial spur) and sclerosis of the greater tuberosity of the humerus. Magnetic resonance imaging (MRI) will demonstrate changes in the supraspinatus tendon and many times there will be evidence of swelling and fluid. If the clinical symptoms are present and a subacromial spur is demonstrable on the plain films, the only additional imaging modality that may be necessary is another plain film of the subacromial region in the anteroposterior projection, with an x-ray tube tilt of 15 degrees in the cephalad direction which would separate the posterior portion of the acromion allowing a better view of the spur. If a subacromial spur cannot be demonstrated and clinical symptoms still indicate an impingement syndrome, a MRI of the shoulder may be necessary to demonstrate the more subtle types of shoulder impingement syndrome.
The treatment of the impingement syndrome depends on the chronicity of the disorder and associated abnormalities. In many patients, especially young athletes, the syndrome is first recognized at the stage of rotator cuff tendinitis and will generally respond well with conservative care. In the more chronic cases in which large subacromial spurs have caused a rotator cuff tear, anterior acromioplasty may be required.
Diagram of the x-ray position for demonstrating the acromioclavicular joint and subacromial spur.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.