The most common form of arthritis is osteoarthritis, also known as degenerative joint disease. Osteoarthritis is seen primarily, but not exclusively, in the elderly. Surveys have indicated that over 40 million Americans have osteoarthritis, including 80 percent of persons over the age of 50.
It is believed that the cumulative effects of decades of joint use leads to degenerative changes. This damage is compounded by a decreased ability to repair joint structures. As we age, there is a decreased ability to restore and manufacture normal joint structures such as cartilage.
The weight-bearing joints, like the knees and hips and joints of the hands, are the joints most often affected with osteoarthritis. In affected joints, there is much cartilage destruction followed by hardening and the formation of large bone spurs in the joint margins. Pain, deformity, and limitation of motion in the joint results.
The onset of osteoarthritis can be very subtle, morning joint stiffness is often the first symptom. As the disease progresses, there is pain on motion of the involved joint that is made worse by prolonged activity and relieved by rest.
Current Medical Treatment: More Harm than Good?
Research is indicating that current drugs being used in osteoarthritis may be producing short-term benefit, but actually accelerating the progression of the joint destruction. Based on data collected from the earliest signs of osteoarthritis to the most advanced stages suggest that cellular and tissue response is purposeful and is aimed at repair of the damaged joint structure. The process contributing to osteoarthritis appears to be able to be stopped and sometimes reversed1. Therefore, the major goal of therapy appears to be enhancing repair processes by various connective tissue cells. Unfortunately, the current medications being used actually inhibit repair processes.
Several studies have attempted to determine the "nature course" of osteoarthritis.1,2 That is the course of the disease if no treatment is given. In one study of the natural course of osteoarthritis of the hip over a 10 year period, all subjects had changes suggestive of advanced osteoarthritis, yet the researchers reported remarkable clinical improvement and x-rays confirmed recovery of the joint space in 14 of 31 hips.2 The authors of the study purposely applied no therapy and regarded their results as reflecting the natural course of the disease. Nearly half of the patients had confirmed recovery without any therapy.
These results, as well as others, raise some interesting questions. Does medical intervention in some way promote disease progression? Can nutrition and various natural therapies enhance the body's own response towards health? The answer to both of these questions appears to be yes.
Aspirin and Other Non-Steroidal Anti-Inflammatory Drugs
The first drug generally used in the treatment of osteoarthritis is aspirin. It is often quite effective in relieving both the pain and inflammation, and is relatively inexpensive. However, since the therapeutic dose required is relatively high (two to four grams per day), toxicity often occurs. Tinnitus (ringing in the ears) and gastric irritation are early manifestations of toxicity.
Other non-steroidal anti-inflammatory drugs (NSAIDs) are often used as well, especially when aspirin is ineffective or intolerable. The following are representative of this class of drugs: ibuprofen (Motrin, Advil, Nuprin), fenoprofen (Nalfon), indomethacin (Indocin), naproxen (Naprosyn), tolmetin (Tolectin), and sulindac (Clinoril). These drugs are also associated with side effects including gastrointestinal upset, headaches, and dizziness, and are therefore recommended for only short periods of time.
One side effect of aspirin and other NSAIDs that is often not mentioned is their inhibition of cartilage repair and acceleration of cartilage destruction. Since osteoarthritis is caused by a degeneration of cartilage it appears that while NSAIDs are fairly effective in suppressing the symptoms, they possibly worsen the condition by inhibiting cartilage formation and accelerating cartilage destruction. This has been upheld in studies which have shown that NSAIDs use is associated with acceleration of osteoarthritis and increased joint destruction.3-6 Simply stated, aspirin and other NSAIDs appear to suppress the symptoms by accelerate the progression of osteoarthritis. Their use should be avoided.
Glucosamine Sulfate: A Natural Alternative to Arthritis Medications
If current arthritis medications should be avoided, what is an arthritis sufferer to do? A naturally occurring substance found in high concentrations in joint structures appears to be nature's best remedy for osteoarthritis. This compound is glucosamine.
In the body, the main action of flucosamine on joints is to stimulate the manufacture of cartilage components. In other words, glucosamine is responsible for stimulating the manufacture of substances necessary for joint repair. This action alone suggests a therapeutic role in osteoarthritis. But, there is much more. Glucosamine has also been shown to exert a protective effect against joint destruction and, when given orally as glucosamine sulfate, it is selectively taken up by joint tissues to exert a powerful therapeutic effect in osteoarthritis.2
Numerous double-blind studies have shown glucosamine sulfate to yield as good as or even better results compared to NSAIDs in relieving the pain and inflammation of osteoarthritis.8-11 What is amazing about these results is that glucosamine sulfate exhibits no pain relieving effects. While NSAIDs offer purely symptomatic relief and may actually promote the disease process, glucosamine sulfate addresses the cause of osteoarthritis. By getting at the root of the problem, glucosamine sulfate not only improves the symptoms including pain, it also helps the body repair damaged joints. This is outstanding, but what is even more outstanding is the safety and the lack of side effects associated with oral glucosamine sulfate. In contrast, the side effects and risks associated with NSAIDs currently used in the treatment of osteoarthritis are significant. The therapeutic margin, a measure of safety, is 10-30 times more favorable for glucosamine sulfate than for commonly used NSAIDs and no adverse side effects have been reported.7
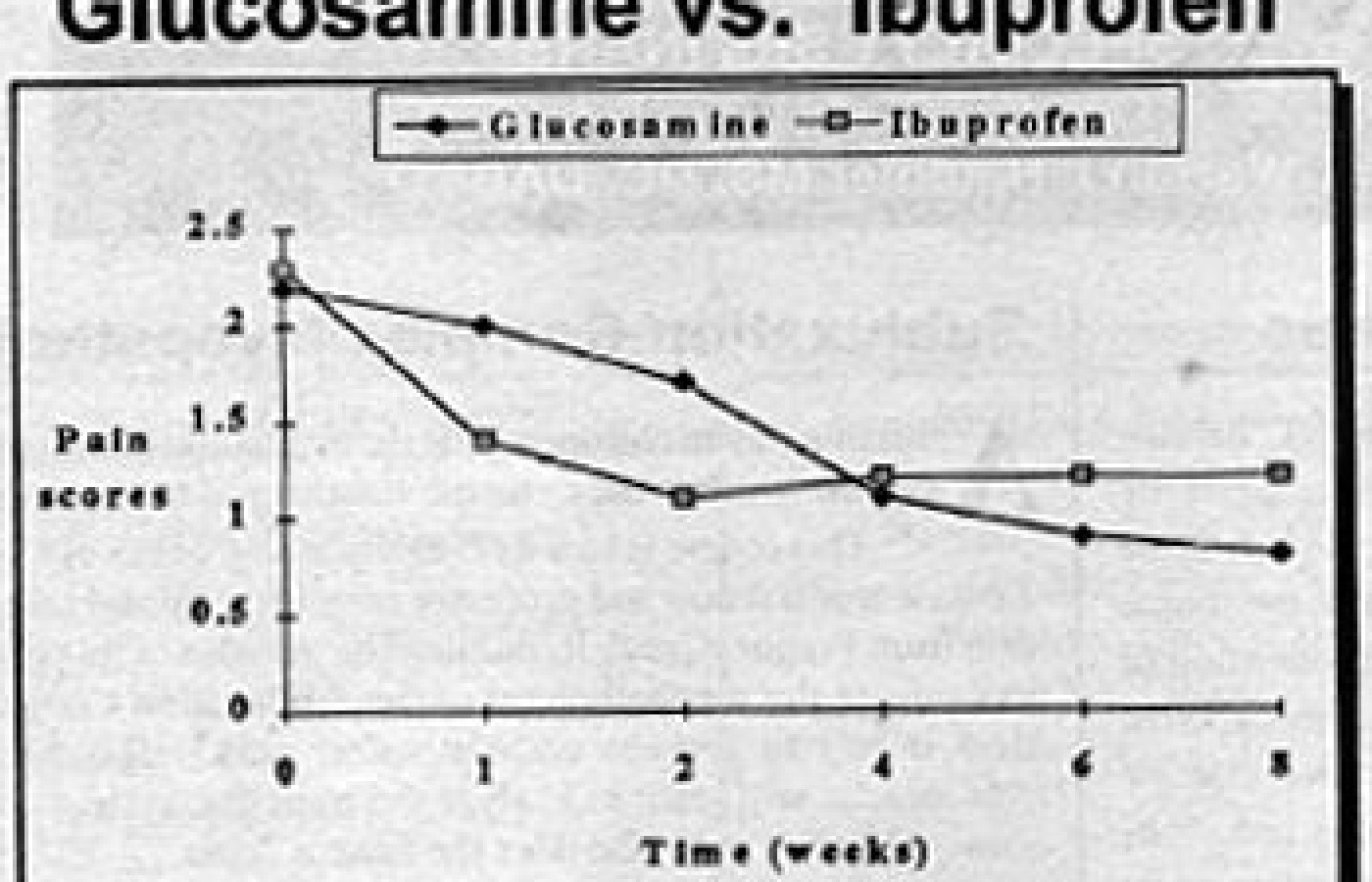
The beneficial results with glucosamine are more obvious the longer it is used. Because glucosamine sulfate is not a pain relieving substance per se, it takes a while longer to produce results. But, once it starts working, it will produce much better results compared to NSAIDs. For example, in one study that compared glucosamine sulfate to ibuprofen (Motrin), pain scores decreased faster in the first two weeks in the ibuprofen group, however by week four, the group receiving the glucosamine sulfate was doing significantly better than the ibuprofen group.
Glucosamine Sulfate vs. Chondroitin Sulfate
Glucosamine sulfate is a simple molecule. As its name indicates it is composed of glucose, an amine (nitrogen and two molecules of hydrogen), and sulfur. It serves as the backbone structure to many glycosaminoglycans including chondroitin sulfate.
In contrast to glucosamine, chondroitin sulfate is a very large, complex molecule. Glucosamine sulfate has a molecular weight of 211. Chondroitin sulfate has a molecular weight of over 30,000. Chondroitin sulfate is so large it is virtually impossible for the body to absorb it intact. It must be broken down into smaller units. Chondroitin sulfate is 250 times larger than glucosamine. To put this perspective, for the body it would be the difference between trying to swallow a whole sesame seed versus a whole watermelon. It is simply impossible. Just like the watermelon, chondroitin sulfate must be broken down into smaller pieces to be absorbed. While 98 percent of orally administered glucosamine sulfate is absorbed intact, the absorption rate for chondroitin sulfate is estimated to be between zero and eight percent.12
From a clinical perspective, glucosamine is extremely effective if given orally. In contrast, the effectiveness of oral chondroitin sulfate is a subject of considerable debate. Most of the studies have utilized injectable forms. If chondroitin sulfate is effective orally, it is most likely due to the body breaking down chemical bonds and freeing up glucosamine.
Another analogy would be the difference between crude ore (chondroitin sulfate) and pure gold (glocosamine). While there is gold in crude ore, if you are trying to make jewelry, it is better to use the pure gold. If you are trying to restore joint structures, it is best to use glucosamine sulfate rather than chondroitin sulfate. Once absorbed, glucosamine is preferentially taken up by cartilage and other joint structures where it simulates the manufacture of mucopolysaccharides like chondroitin sulfate.12
Summary
The case of osteoarthritis is a classic example where current medical treatment simply suppresses symptoms, and since it doesn't address the underlying cause, the treatment actually promotes the disease process. The use of glucosamine is a classic example of how a natural substance improves a condition by addressing the underlying cause and supporting the body's ability to heal itself.
References
Bland JH, Cooper SM: Osteoarthritis: A review of the cell biology involved and evidence for reversibility. Management rationally related to known genesis and pathophysiology. Sem Arthr Rheum 14:106-33, 1984.
Perry GH, Smith MJG, Whiteside CG: Spontaneous recovery of the hip joint space in degenerative hip disease. Ann Rheum Dis 31:440-8, 1972.
Brooks PM, Potter SR and Buchanan WW: NSAID and osteoarthritis -- help or hindrance. J Rheumatol 9:3-5, 1982.
Newman, NM, Ling, RSM: Acetabular bone destruction related to non-steroidal anti-inflammatory drugs. Lancet: ii; 11-13, 1985.
Solomon L: Drug induced arthropathy and necrosis of the femoral head. J Bone Joint Surg 55B:246-51, 1973.
Ronningen H, Langeland N: Indomethacin treatment in osteoarthritis of the hip joint. Acta Orthop Scand 50:169-74, 1979.
Setnikar I, Pacini A, Revel L: Antiarthritic effects of glucosamine sulfate studied in animal models. Arzneim-Forsch 41:542-5, 1991.
Vaz AL: Double-blind clinical evaluation of the relative efficacy of ibuprofen and glucosamine sulfate in the management of osteoarthrosis of the knee in outpatients. Curr Med Res Opin 8:145-9, 1982.
Crolle G, D'este E: Glucosamine sulfate for the management of arthrosis: a controlled clinical investigation. Curr Med Res Opin 7:104-14, 1980.
Tapadinhas MJ, Rivera IC, Bignamini AA: Oral glucosamine sulfate in the management of arthrosis: report on a multi-center open investigation in Portugal. Pharmatherapeutica 3:157-68, 1982.
D'Ambrosia ED, Casa B, Bompani R, Scali G, Scali M: Glucosamine sulphate, a controlled clinical investigation in arthrosis. Pharmatherapeutica 2:504-8, 1982.
Setnikar I, Giachetti C, Zanolo G: Pharmacokinetics of glucosamine in the dog and in man. Arzneim Forsch 36:729-35, 1986.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.