Calcium, in searching for fame and fortune, must have hired the best of press agents. Calcium has become a buzzword, a multibillion dollar industry, and a legend in its own time. Even medical doctors, who historically belittled the use of vitamins or mineral supplements, now regularly will prescribe calcium.
The item that has spurred such widespread use of calcium is osteoporosis. The popular notion that osteoporosis is a calcium deficiency disease (or an estrogen deficiency) is naive. Yes, calcium is required in human nutrition and physiology. Yes, calcium is a component of bone. But is it realistic to expect that calcium eaten as food or supplement necessarily becomes bone? Life is not this simple.
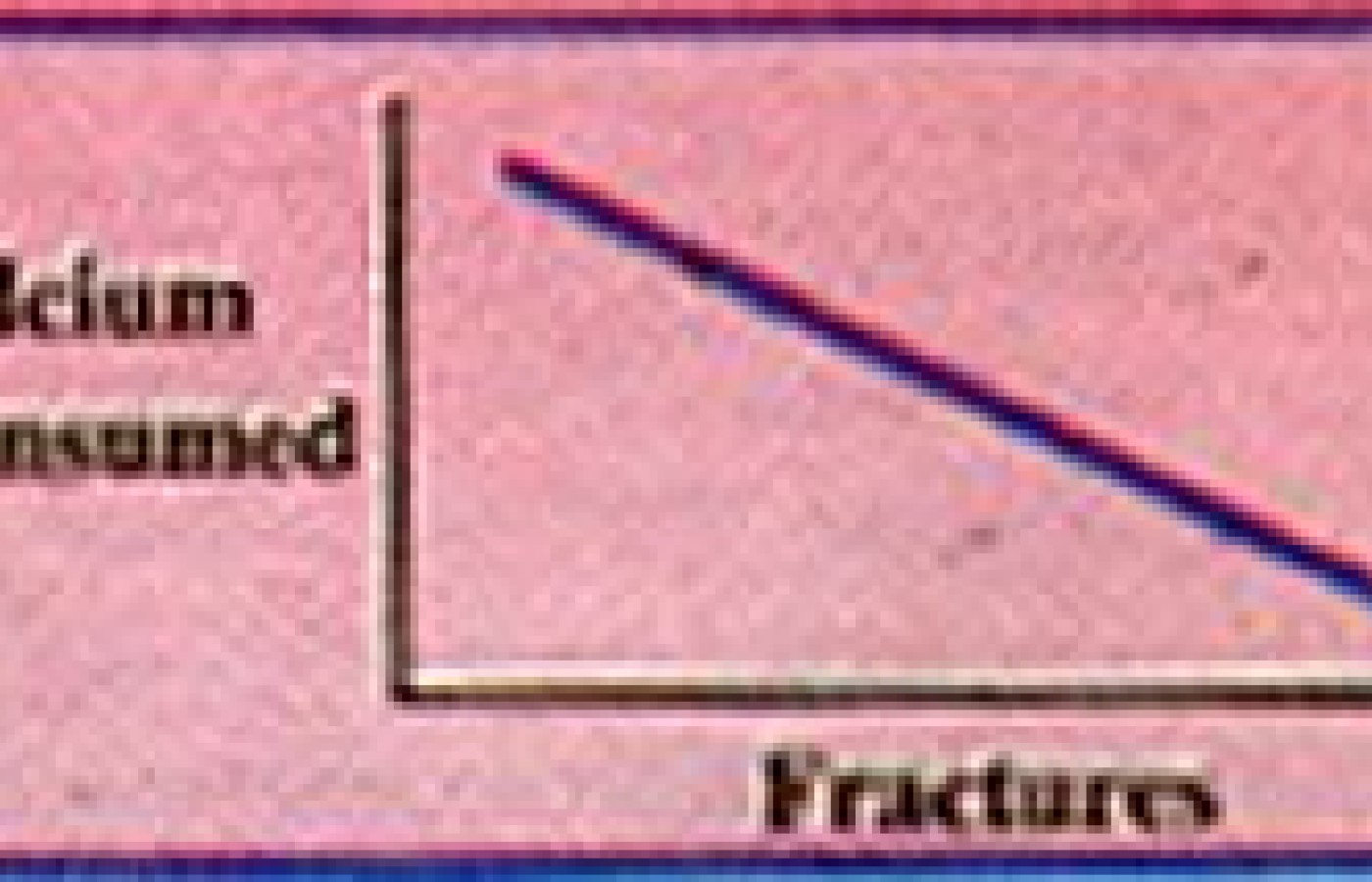
If life were this simple, we would expect to see a direct positive correlation between calcium consumption and bone mass or a negative correlation between calcium consumption and fractures due to osteoporosis. Graphing this relationship would look like this:
Reality is far form this. In fact, there are no data available that show this relationship. What is seen is a random pattern showing no correlation between calcium consumption and incidence of hip fracture.
Singapore, where calcium consumption approximates 600 mg/day, has only 10 percent of the hip fractures compared to the U.S., where approximately 1000 mg/day of calcium is consumed. Hong Kong, consuming 400-500 mg/day, has 30 percent the fracture rate of the U.S. Finland, consuming 1400-1500 mg/day of calcium, has 50 percent of the hip fracture rate of the U.S., and nearly five times the rate of Singapore.1
From Hegsted
In view of these epidemiologic data, it is clear that increased calcium consumption does not correlate with a decrease in hip fractures. Yet the "increase the calcium" recommendations are made by the dairy council, certain antacid manufacturers, vitamin companies, and many health care practitioners.
The bottom line: calcium is not the whole story. Still the USRDA for calcium is 800 mg/day for most adults and 1200 mg/day for pregnant and lactating women. A 1984 consensus conference on osteoporosis recommends 1000 mg/day for estrogen replete women and 1500 mg/day for estrogen deprived women.2 These numbers contrast with the World Health Organization's "practical allowance" of 400-500 mg/day.
In the U.S., we continue to pour on the calcium in the form of dairy products and supplements. Calcium consumption has mistakenly become the goal and the assumed safe haven. In truth, we're trying to build a healthy skeleton.
When building any product or body tissue, one must acquire all the necessary raw materials. Our overemphasis with calcium is like trying to build a house with only lumber being delivered. How about nails, or roofing, or a foundation?
We should listen less to the dairy council and other promoters of calcium overconsumption and pay attention to the habits of the people in Singapore. Our goal is to build and or maintain a health and robust skeleton. To achieve this end, we do need some calcium. We also need other minerals, vitamins, exercise, less protein than we think, avoidance of certain drugs, etc.
Future articles will address the myriad of considerations regarding osteoporosis and nutrition, diagnosis, medical treatments, and chiropractic treatment.
References
Hegstead DM. Calcium and osteoporosis. J Jutr 1986, 116:2316-9. 1986
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.