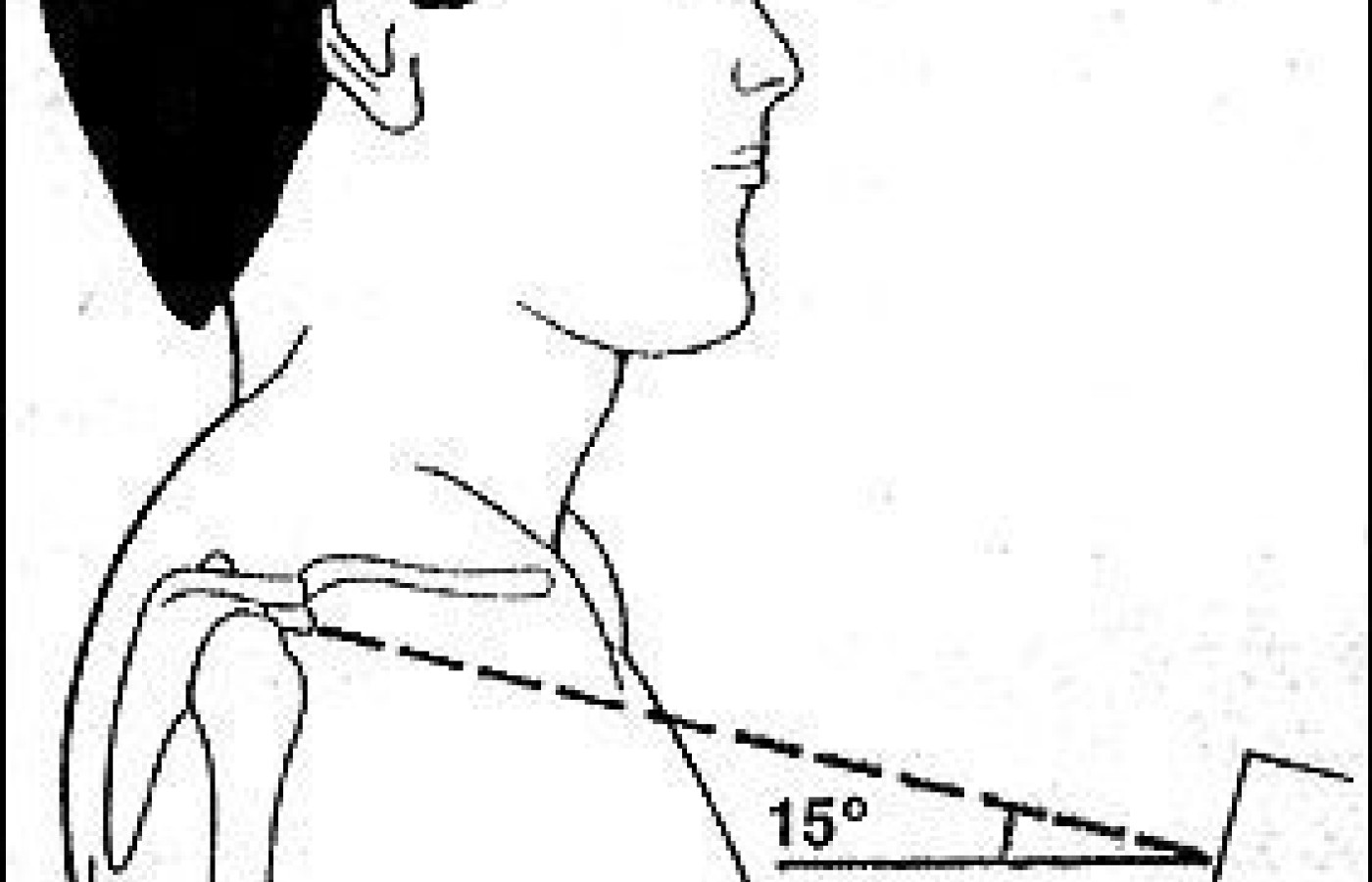
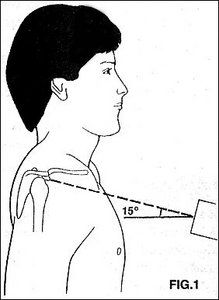
The shoulder girdle is a rather complicated structure to evaluate on plain films. Small fractures and mild degenerative changes can be overlooked on a standard shoulder series. Among the areas commonly overlooked or difficult to evaluate is the acromioclavicular joint, which is often "burnt out" or over-penetrated on the shoulder series. The best way to evaluate the acromioclavicular articulation is with an angled view and a slightly decreased x-ray technique. Figure 1 demonstrates the positioning for this view. The patient is standing with the arm in the neutral position and the central beam is directed 15o cephalad toward the clavicle. As over-exposure of the film is common, reduce the radiographic factors by about 33 percent from the standard AP shoulder view.
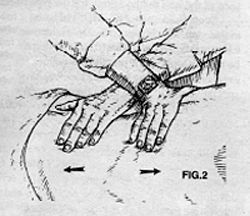
Another area that is difficult to evaluate on a standard shoulder series is the glenoid fossa. It generally is overlapped by the head of the humerus. The good view for evaluating the glenoid is by positioning the patient as in Figure 2, where the patient is angled about 40o toward the side of interest and the central beam is directed toward the glenohumeral joint. Another structure which is difficult to evaluate is the scapula.
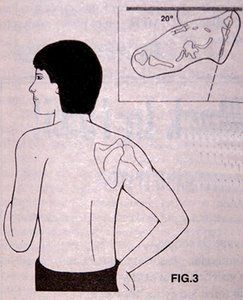
Figure 3 demonstrates the patient positioning for the trans-scapular or Y view of the shoulder. The patient faces the buckey and is rotated about 20o from the buckey, with the shoulder of interest closest to the buckey. The arm on the side of interest is slightly abducted and the elbow flexed. In other words, put the patient's hand on their hip. The central beam is directed toward the medial border of the protruding scapula. There are many more complicated views of the shoulder but these are very easy to perform, even if the patient is symptomatic. If there is still a question of pathology, even with these extra views, special studies may be necessary.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.