The term "osteochondrosis" has traditionally been used to describe a group of disorders that share certain features: predilection for the immature skeleton; involvement of an epiphysis, apophysis, or epiphysioid bone; and a radiographic picture that is dominated by fragmentation, collapse, sclerosis, and frequently, reossification with reconstitution of the osseous contour. In the past it was thought that this group of conditions were heterogenous and due to a primary impairment of local arterial supply that led to osteonecrosis. It is now apparent that there are many dissimilarities and that they are not all associated with osteonecrosis.
It is now recognized that osteonecrosis is not a factor in some of the osteochondroses (e.g., Blount's tibia vara and Scheuermann's disease), and that in others, aseptic bone necrosis is not a primary event, but appears to follow a fracture or other traumatic insult (e.g., Keinbock's disease of the lunate bone). Some of the osteochondroses are not disorders at all but appear to represent variations in normal ossification (e.g., Sever's disease of the calcaneus).
It is best to classify these disorders into three types: articular osteochondroses, nonarticular osteochondroses, and physeal osteochondroses. The articular osteochondroses are characterized by initial deformity of the developing epiphysis with the potential for subsequent alteration of the joint itself. These articular osteochondroses can be further divided into two subtypes. The initial epiphyseal deformity can be due to irregularity of endochondral ossification involving the articular and growth cartilage or secondary to ischemic necrosis. Both types (chondrogenesis and osteogenesis) are affected.
The nonarticular osteochondroses involve tendinous and ligamentous attachments to apophyses as in Osgood-Schlatter disease, Sinding-Larsen-Johansson disease or Sever's disease. In some instances, they can occur in response to abnormal pressure or chronic stress, which will alter the normal chondrogenesis and osteogenesis. As for the physeal osteochondroses, Blount's disease or Scheuermann's disease relate to abnormalities of the longitudinal growth plate in either the appendicular or axial skeleton.
The following chart lists the most common osteochondroses and their probable mechanism.
Femoral head Metatarsal head Carpal lunate Tarsal navicular Capitulum of humerus Phalanges of hand Tibial tuberosity Proximal tibial epiphysis Discovertebral junction Patella Calcaneus Ischiopublic synchondrosis
Osteonecrosis, perhaps due to trauma Osteonecrosis due to trauma Osteonecrosis due to trauma Osteonecrosis or altered sequence of ossification Osteonecrosis due to trauma Osteonecrosis, perhaps due to trauma Trauma Trauma Trauma Trauma Normal variation is osteonecrosis Normal variation is osteonecrosis
(Chart obtained from Resnick & Niwayama. Diagnosis of Bone and Joint Disorders, p. 3289)
Disorders Associated with Primary or Secondary Osteonecrosis
Legg-Calve-Perthes disease primarily affects children between 4 and 8 years old. The disorder is more frequent in boys with one hip being affected; occasionally both are affected (about 10 percent of the time). The clinical signs are limping, pain and limitation of motion of the affected hip. These clinical symptoms are neither prominent nor constant and may persist for only a few days or weeks. At other times, more prolonged signs are detected, and atrophy of the soft tissues, muscle spasm and contracture may be present. Occasional radiographic changes are present without clinical symptoms. In other words, the clinical picture will vary greatly. The possibility of Legg-Calve-Perthes disease must be considered in a child with acute manifestations in the hip, or in a child with chronic hip complaints.
The most common radiographic findings associated with Legg-Calve-Perthes disease are fissuring and fracture of the femoral ossific nucleus, and flattening and sclerosis of the femoral ossification nucleus. Fragmentation and compaction of the subchondral bony fracture debris lead to the development of a subchondral lucent area along the fracture line called the crescent sign. The femoral head will begin to collapse and the epiphysis will appear sclerotic. The progression and extent of disease are highly variable. The epiphysis can reconstitute and there will be a complete remodeling of bone and complete recovery. More often, however, the child is left with a mushroom-shaped femoral head and a foreshortened femoral neck.
The etiology of Legg-Calve-Perthes disease is generally thought to be vascular insufficiency to the femoral head, but it is not precisely understood what causes the deficiency of blood supply.
Freiberg's infraction is a disorder affecting females (13-18 years) more frequently than males. Clinical symptoms consist of local pain, tenderness, swelling and limitation of motion of the corresponding metatarsophalangeal joint. Radiographic abnormalities appear similar to the features described in Legg-Calve-Perthes disease. The metatarsal head may completely remodel, but more often the metatarsal is foreshortened due to early closure of the growth plate. The etiology of Freiberg's infraction is felt to be due to the wearing of high heeled shoes at an early age.
Keinbock's disease is a peculiar affliction of the carpal lunate. It is most commonly observed in patients between 20 and 40 years old, and has a predilection for the right hand in individuals engaged in manual labor. The etiology of this condition is not clear. It is felt to be related to trauma; however, certain anatomic and biomechanical features of the lunate may predispose this bone to injury and subsequent osteonecrosis.
Kohler's disease is a disorder more frequent in boys between the ages of 3 and 7. Clinical manifestations may be quite mild, consisting of local pain, tenderness, swelling and decreased range of motion. Radiographically there are changes similar to Legg-Calve-Perthes disease. Fragmentation and sclerosis of the navicular may occur; over a period of 2 to 4 years the navicular may regain its normal appearance.
Panner's disease of the capitulum of the humerus is very rare and resembles Legg-Calve-Perthes disease. Boys are almost exclusively affected between the ages of 5 and 10 years. The clinical manifestations are typically mild and recovery is frequent.
Thiemann's disease usually affects teenaged boys and is associated with painless swelling of proximal interphalangeal articulations, digital shortening and deformity. The disease is familial, probably transmitted as a dominant trait. Radiographs reveal irregularity of the epiphyses of the phalanges, especially in the middle fingers. The epiphyses appear sclerotic and fragmented and may contain medial and lateral osseous excrescences. Eventually, the joint space becomes narrowed, the base of the phalanx thickens and phalangeal shortening is seen.
Disorders Related to Trauma or Abnormal Stress without Evidence of Osteonecrosis
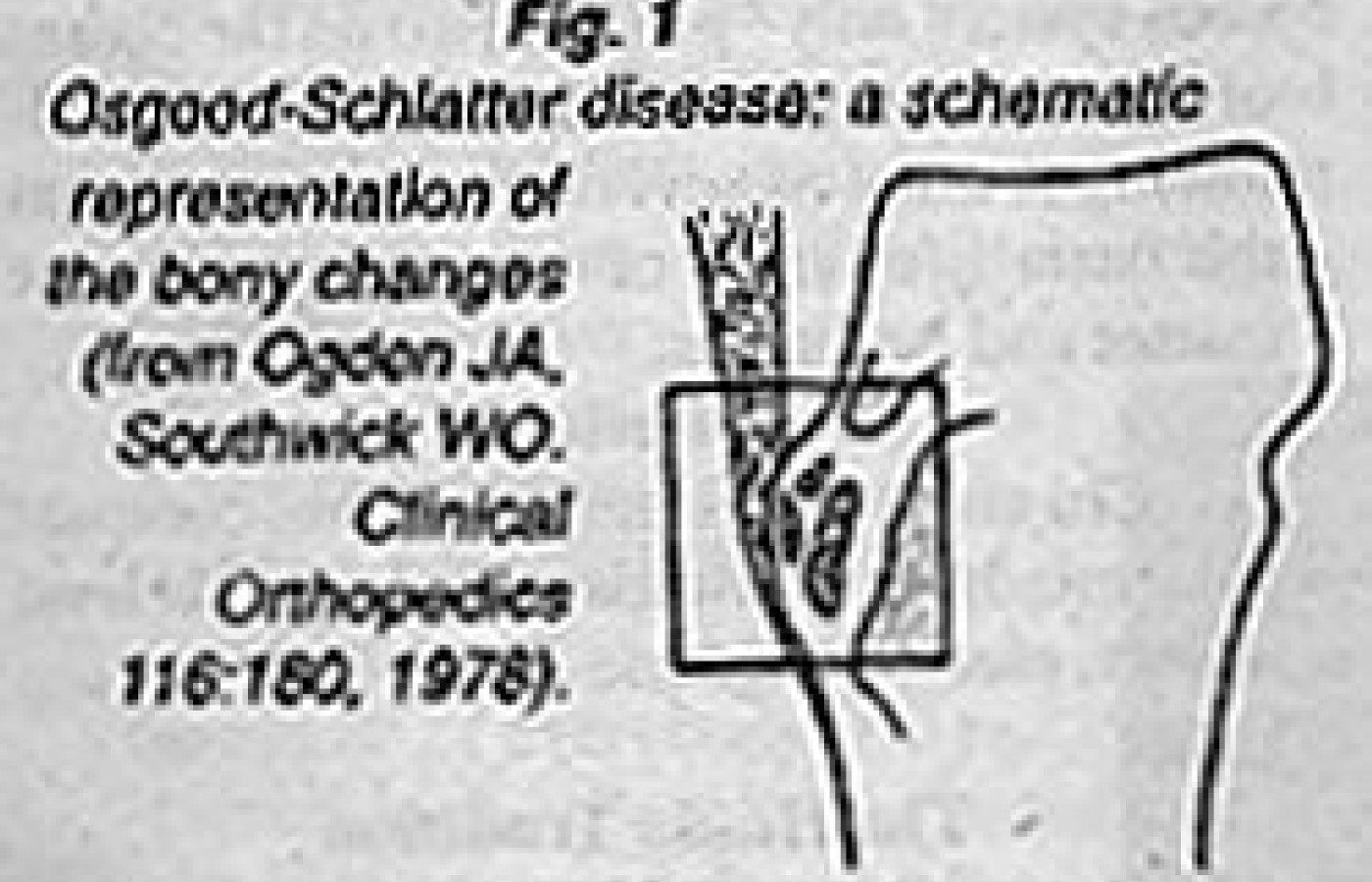
Osgood-Schlatter disease is considered to be a disorder caused by chronic or acute trauma. It occurs in adolescents between the ages of 11 and 15. It is usually associated with a history of participation in sports that involve kicking, jumping, and squatting. A rapid growth spurt is also often associated with onset of symptoms. The radiographic abnormalities in this disease are influenced by the age of the patient. Initially soft tissue in from the tuberosity results from edema of the skin and subcutaneous tissue. If the tuberosity is entirely cartilaginous in structure, no change will be detected in it initially, but examination 3 or 4 weeks later may show single or multiple ossific collections in the avulsed fragment. In the older child in whom the ossification center has begun to develop, one or more foci of radiopacity can be recognized in the vicinity of the tubercule; the latter protuberance may have surface irregularities marking the site from which fragments of cartilage and bone have been avulsed (see Figure 1). Eventually, the radiographic appearance may revert to normal, although persistent ossific fragments may be present to mark the site of previous disease.
Blount's disease is a local disturbance of growth of the medial aspect of the proximal tibial epiphysis. There are two types, infantile and adolescent; the infantile is by far the more common form. It occurs in children aged 1-3 years. This disorder appears to be caused by persistence of the normal physiologic bowing in infants rather than disappearing progressively to a straight leg as the bowing remains. This causes stress on the knee joint as the child becomes heavier and walks more. Clinically the affected children may be early walkers.
Progressive bilateral bowing of the legs during the first year of life is difficult to differentiate from physiologic changes. The tibia may be angulated acutely inward just below the knee, and a non-tender bony protuberance can be palpated along the medial aspect of the proximal tibia. The fibular head may also be prominent. Pain is not evident. Associated findings are obesity, shortening of the leg, tibial torsion, and pronated feet. The radiographic findings simulate exaggerated physiologic bowing. The tibia is in varus position. There is a depressed medial tibial metaphysis with an osseous excrescence or spur. The severity of the osseous changes are highly variable.
Scheuermann's disease generally affects individuals between the ages of 13 to 17. Clinical manifestations are highly variable. In some individuals the disease is totally asymptomatic; others may experience fatigue, defective posture, aching pain aggravated by physical exertion and tenderness to palpation. An increase in the thoracic kyphosis is a common finding. On radiographs, irregularity of the vertebral contours is evident. The degree of irregularity will vary, but when severe can be accompanied by disc height loss and vertebral body wedging.
(Fig. 2: Diagram of Scheuermann's disease. The underlying abnormality relates to intraosseous displacement of disc material through the cartilaginous endplate (A). This produces radiolucent lesions of the vertebral bodies with surrounding sclerosis, intervertebral disc space narrowing, and irregularity of the vertebral body contour (B). From: Resnick & Niwayama. Diagnosis of Bone and Joint Disorders, p. 3322).
The main radiographic feature of this disorder is cartilaginous nodes. It has been determined that cartilaginous nodes are due to an endplate fracture resulting from failing under dynamic load in compression or shear at a time when the plate and the metaphysis are vulnerable as a result of rapid growth. Nuclear protrusions occur through the weakened endplates, and the prolapsed disc material becomes surrounded first by a cartilaginous casing and later by an osseous one. The cartilaginous nodes eventually consist of both nucleus pulposus and annulus fibrosus. Fibrovascular proliferation and narrowing of the intervertebral disc can ensue.
Sinding-Larsen-Johansson disease generally affects adolescents between 10 and 14 years of age, consisting of tenderness and soft tissue swelling over the lower pole of the patella, accompanied by radiographic evidence of osseous fragmentation. The lesion is felt to be due to a traction phenomenon in which contusion or tendinitis in the proximal attachment of the patellar tendon can be followed by calcification and ossification, or in which patellar fracture or avulsion produces one or more distinct ossification sites. The natural duration of the disease is approximately 3 to 12 months.
Osteochondroses Due to Variations in Ossification
Sever's disease is a normal variation in the ossification of the secondary ossification center of the calcaneus.
Van Neck disease is a normal variation in the ossification of the ischiopubic synchondrosis. It is now regarded as a very common normal pattern of ossification.
There are at least 5 or 6 other osteochondroses due to variations in ossification that were originally thought to represent osteonecrosis and repair; they all have eponyms and are simply variations in the ossification process. It is best not to review them since they are not disorders, only normal findings. Why memorize eponyms for normal findings? It's better to remember the disorders that cause significant clinical symptoms that may result in future complications.
Reference
Resnick D. Diagnosis of Bone and Joint Disorders. 2nd ed, 1988.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.