About the author: Dr. Blanchard is a chiropractor and professional golfer who has trained thousands of DCs on the biomechanics of golf and treatment of golf injuries.
The primary complaint of patients who play golf is low back pain. This condition can result from an improper pivot, lumbopelvic subluxation and/or inadequate flexibility. When pre-existing physical problems couple with the repetitive, one-sided nature of the golf swing, it's a big problem. This explains why approximately 50 percent of patients who play golf will eventually become injured and need your help.
The Pivot
"Pivot" is defined as a "shaft about which related parts rotate." For the right-handed golfer, the shaft will be the right leg; related parts are the hips and shoulders. There are two key points to understand about a good pivot:
The position of the golfer's feet is the critical starting point for a good pivot. The pivot is essential to buildup kinetic energy (power) into the golf swing. Kinetic energy translates to club head speed, which is necessary to compress the golf ball. The more you compress a golf ball, the farther it goes.
Subluxation
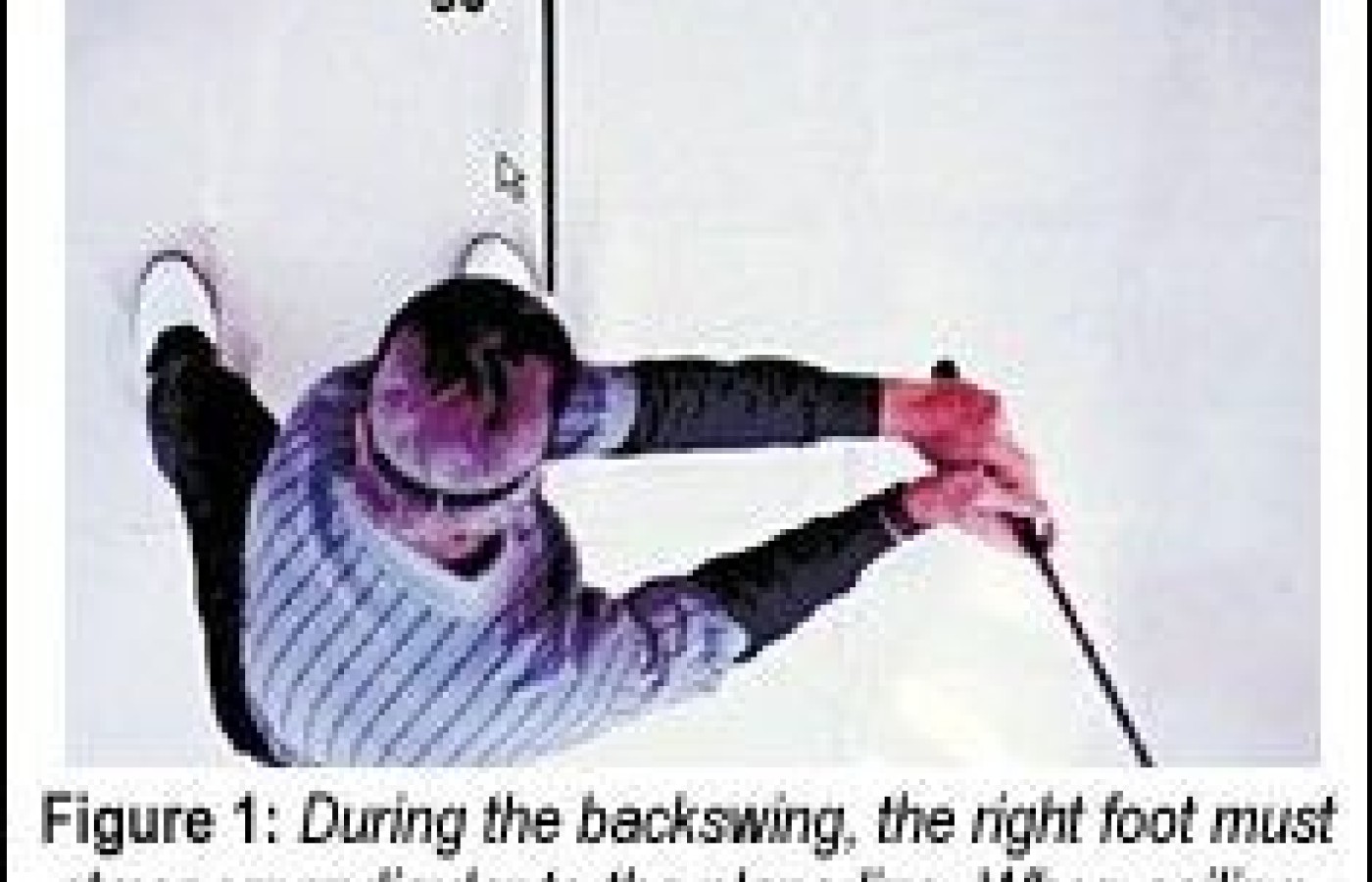
Most patients will not position the right foot perpendicular to the plane line. When they try, they experience pain in the right sacroiliac joint as the hips rotate during the backswing. For relief, they will position their right foot outward so they can make a bigger hip turn with less pain. Unfortunately, with the right foot out of position, there is a loss of power and an inconsistent direction of ball flight.
Don't forget to check the integrity of the secondary curve of the lumbar spine. Without adequate lumbar lordosis, your patients will be at a mechanical disadvantage when they try to swing the club. The lumbar curve is an essential source of mechanical leverage for rotating the hips when swinging at a golf ball. (Refer to Part 1 in the series, "A Therapeutic Treatment and Prevention Program," in DC, December 15, 2001, on line at www.chiroweb.com/archives/19/26/02.html.)
Check your patient for subluxation in the pelvic girdle. For the right-handed golfer, if the right ilium is subluxated anterior-superior (AS), the transfer of body weight into the right ilium during the backswing will require more effort as your patient attempts to coil into a "longer" functional leg. In addition, the coil will be restricted and painful for your patient, since the right ilium will have a problem releasing to receive the transfer of weight into the right hip.
Poor Flexibility
The following positions are both diagnostic and corrective for improving the flexibility around the pelvic girdle. During examination, have your patients assume each stretch position and hold for at least 60 seconds. Make sure they keep breathing. Difficulty getting into position or labored breathing is diagnostic that this stretch is needed.
My next article, Part 4, will cover evaluation, strength and conditioning procedures, and protocols necessary for your patients to stabilize their pivots.
Jeffry Blanchard,DC Encinitas, California jhbdcpga@aol.com www.blanchardgolf.com
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.