Your patient wants to hit the ball as far as possible; it's fun. There are two basic moves to the golf swing: the backswing, which is necessary to build kinetic energy, and the downswing, the release of kinetic energy. Your patient knows a booming drive requires a long, flowing backswing. That movement requires flexibility in the shoulders and hips. It requires an unrestricted ability of the spine to bend laterally, rotate and extend.
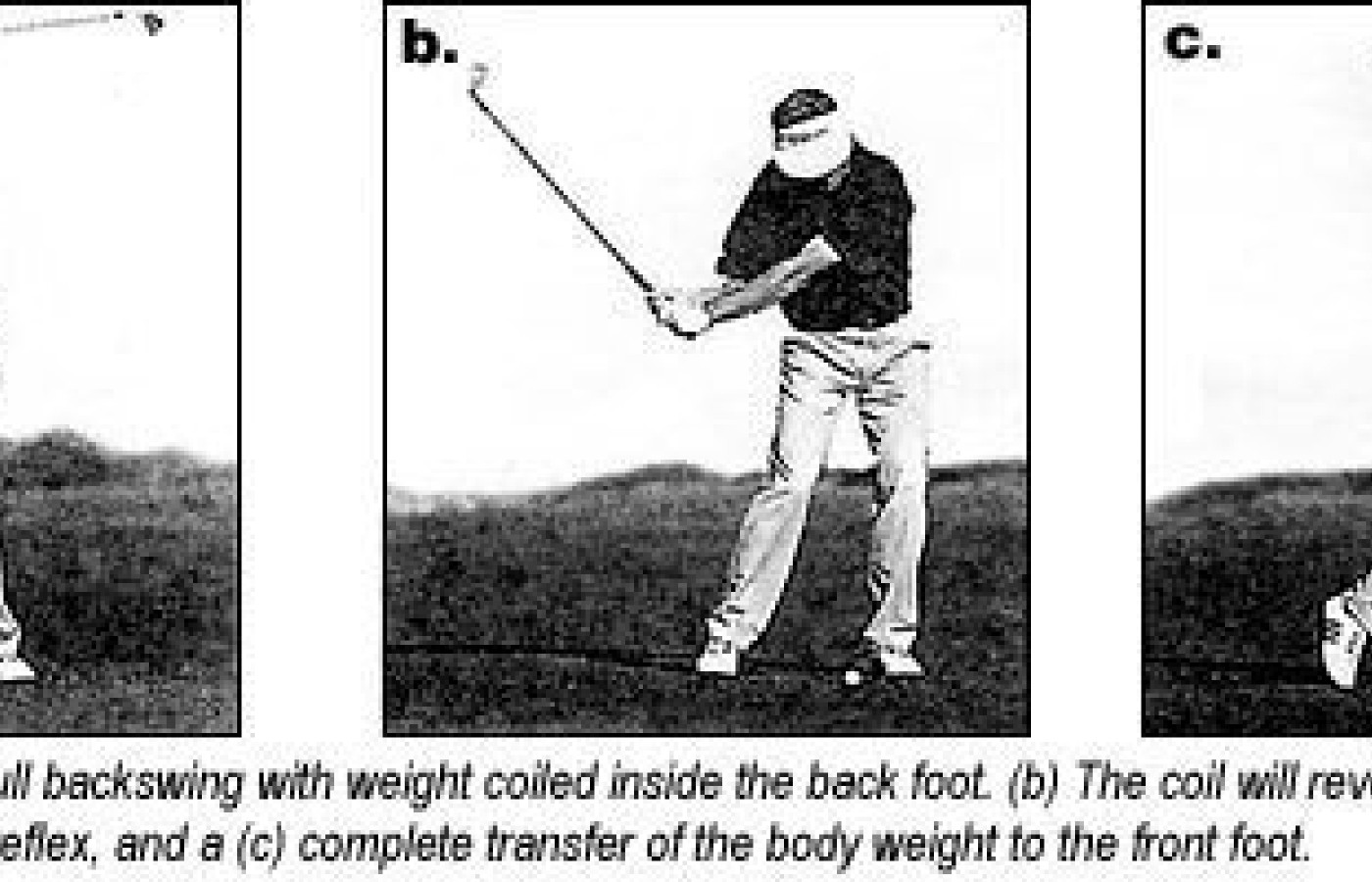
At least 80 percent of your patients lack the necessary flexibility in the shoulders and hips to swing the golf club on track through the necessary planes of motion. In less than 1.5 seconds, the golfer must generate enough kinetic energy to get the club head moving at around 100mph. From a static posture at address, the golfer's body weight is coiled to a point inside the back foot. When the limit of the musculoligamentous elastic barrier is reached, the coil, by reflex, will immediately reverse itself. The downswing starts with the hips. The golfer first slides, then rotates toward the target to make room for the now-released kinetic energy stored in the upper torso, as the forward arm descends the vertical plane. The club head is delivered to the ball on an inside-out path through the transverse plane. As your patient stands tall, facing the intended target, there is a complete transfer of the body weight to the front foot at the finish of the swing.
But where are points of reference for the guidance of this kinetic energy? Once movement begins, how do we know if the body is moving in the proper sequence and direction? In the golf swing, we know for certain that if you wait for the feedback of the flight path of the ball, it is too late. In hitting the ball farther, flexibility of the shoulders and hips are important, but how can this be measured and improved? Adequate range of motion of your patient's shoulders includes the range of motion of the thoracic spine.
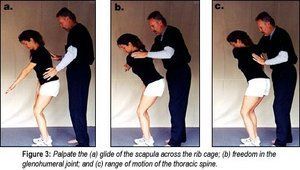
The shoulders and the torso move together, so consider them one functional unit. During the first phase of the backswing in a right-handed golfer, the left scapula should glide freely across the torso. Once the elastic barrier has been reached, the glenohumeral joint will activate to allow continued movement of the left arm up the vertical plane. Once this elastic barrier has been reached, the thoracic spine will complete the necessary rotation as the left arm climbs the vertical plane to "11 o'clock."
The sequence of musculoligamentous motion in the shoulders during the backswing is scapulothoracis, glenohumeral, and thoracic rotation.
Clinical Examination: The Shoulders
We need to establish a point of reference for the movement of the shoulders and torso before we begin the clinical examination. Place a golf ball on the floor. Place a piece of tape on the floor from the ball to 10' behind the ball. This is called the "plane line." It is your reference point of origin for measurement of body movement and positional location of the golf club during the swing.
Without a club in hand, have your patient assume the posture used to address the ball. Feet, hips and shoulders must be parallel to the plane line.
Place the back of the patient's right hand on the right hip pocket.
Extend the patient's left elbow so the left arm is pointing to "six o'clock."
Guide your patient's left arm up the vertical plane and parallel to the plane line to the limit of the elastic barrier of the scapula as it glides outward across the upper torso. Palpate for any motion restrictions.
As the left arm continues to climb the vertical plane, palpate for any motion restriction at the glenohumeral joint when it engages.
Palpate for any motion restriction in the thoracic spine when it engages to rotate, after the glenohumeral joint reaches the limit of its elastic barrier.
Do not be surprised at the limitation of your patient to push the left arm up the vertical plane past "nine o'clock." The average tour professional can reach to "11 o'clock" without postural compromise. The biggest hitters on tour reach noon on the dial. It is important that your patient keeps the left arm extended on the vertical plane and parallel to the plane line. Your patient should not be allowed to lift the head and torso during the exam. The goal is to try and duplicate the movement of the golf swing.
Bending the left elbow, lifting the head or torso, or movement of the left arm into the transverse plane is a compensatory move for a lack of shoulder and upper torso flexibility.
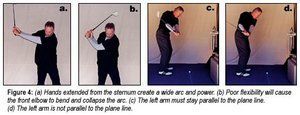
Patients know they have to take a long backswing to generate greater power and distance. But 80 percent of people lack the necessary flexibility in the scapula and glenohumeral joint, so they compensate by bending the front elbow in response to this lack of flexibility. The width of the arc will collapse, resulting in a significant loss of club head speed and power. They will pull the front arm inside, in the plane line response to lack of rotation in the thoracic spine.
Once the left arm pulls into the transverse plane during the backswing, it has to go back through the same plane during the downswing. In the golf swing, this is a prescription for disaster! Only the club head should be traveling through the transverse plane, not the left arm. The left arm should move down the vertical plane.
Correction Protocol
Scapulathoracic Restriction: To increase the range of motion of the scapular glide across the rib cage, elbow curls are useful. (See Figure 5)
The patient may stand or sit, with knuckles placed to the temples with palms facing out.
Contract the rhomboid and squeeze the scapula together. Imagine their medial borders touching.
Separate the scapula by hinging the forearms forward until the elbows touch in front of the chin. Do not let the wrists bend.
Perform three sets of 10.
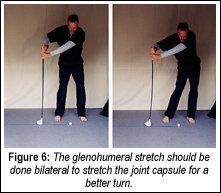
Glenohumeral Restriction: An increase in the range of motion of this joint capsule is difficult, but the following exercise is useful. You may want to try this yourself to understand your patients' perspective.
Stand at address with your feet, knees, hips and shoulders parallel to the plane line.
Place the head of your driver on the plane line about 18" outside your back foot. Place your right thumb on the top of the grip with the back of your hand facing the target.
Reach back with your left hand and take hold of the grip just below your right hand. The back of your left hand should be facing just as it would during a normal golf swing.
Push with your right hand away from the target and pull with your left hand toward the target. Let you hips turn toward the target. Feel the pull at the glenohumeral joint.
Hold the stretch for 60 seconds. Don't forget to breathe.
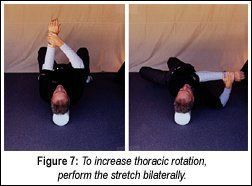
Thoracic Rotation: In addition to spinal adjustments, add the following stretch to increase thoracic range of motion. Your patient will need a six-inch round thoracic roller made of foam. Again, trying this first will help you better understand the procedure.
Sit at one end so your entire spine and head are on top of the roller.
With knees bent, spread your feet about hip-width apart for balance. Extend your arms straight up from your supine torso. Place your palms together.
Place your right hand over your left wrist and pull your left arm across your torso like you would during the backswing. Let your knees go left as your arms go right. Feel the rotation in the thoracic spine.
Repeat five times each way.
In the next segment, we will continue to concentrate on the backswing, with a look at lumbopelvic function.
Jeffry Blanchard,DC Encinitas, California jhbdcpga@aol.com Blanchardgolf.com
Leonard Finkel Vista, California glfgd@aol.com www.golfandlife.com
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.