The Big Toe's Connected to the... Don't Ignore Hallux Valgus
Jeffrey Tucker, DC, DACRB
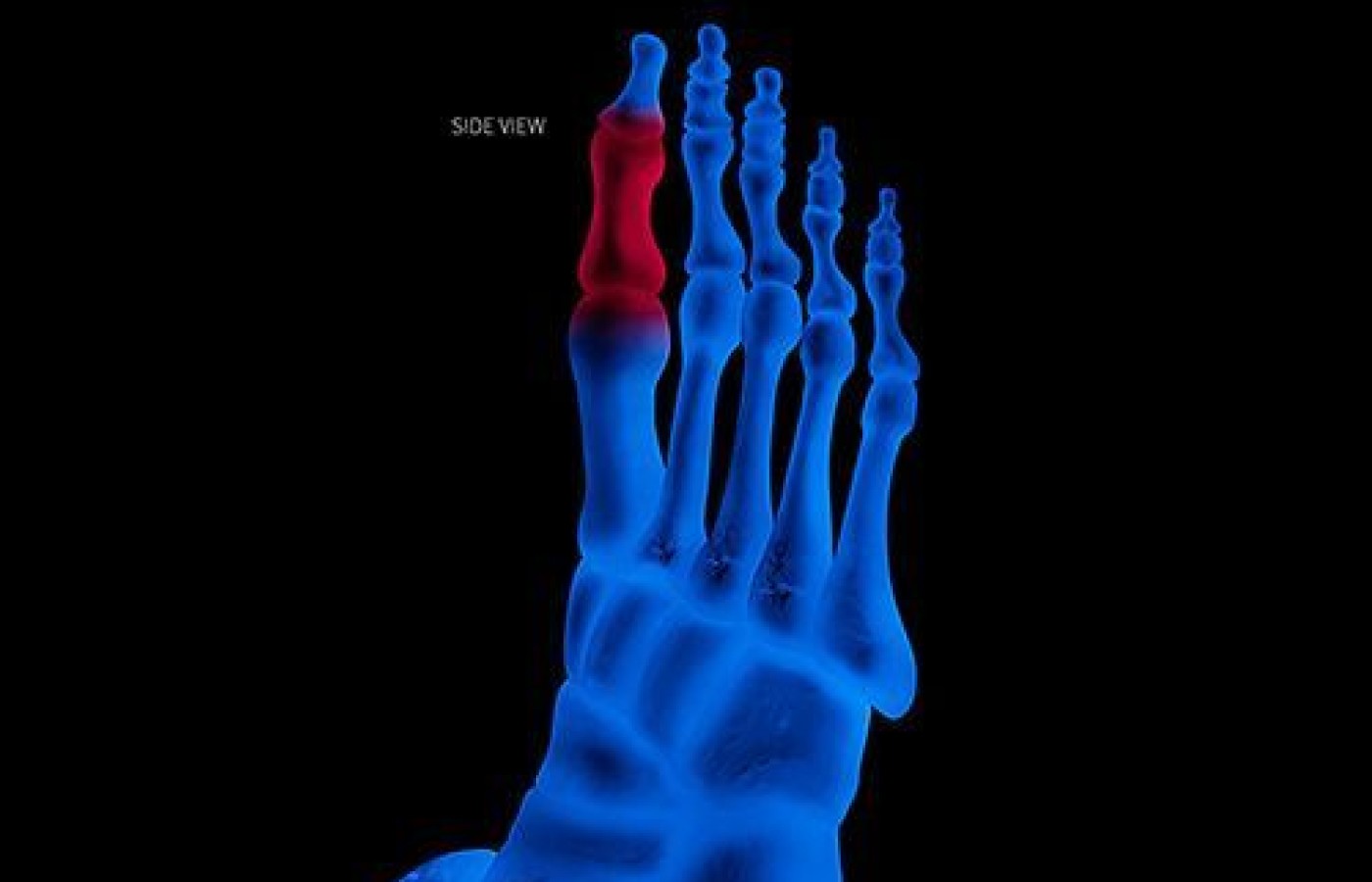
A bunion consists of a thickened callus, an inflamed adventitious bursa and a bony exostosis forming at the dorsomedial aspect of the first metatarsal head. Even with small angles of deformity, I know that over time these are probably going to hurt or cause some gait dysfunction later in life that will influence other body parts.
Therefore, I think we have a responsibility to point out this condition to patients and discuss some simple interventions for good foot hygiene; with the hope that we can alter the course of this deformity.
Signs & Symptoms: What to Look For
A bulging bump on the outside of the base of the big toe
Swelling, redness or soreness around the big toe joint
Corns or calluses, often where the first and second toes overlap
Persistent or intermittent pain in the area of the big toe
Restricted movement of the big toe if arthritis affects the toe
Bunions can lead to other painful foot problems such as hammertoes, bursitis, bunionnettes or painful balls of the feet.
Bunions are not typically patients' chief complaint when they come and see me. I notice the big-toe deformity when I do my static postural analysis and that's often when the conversation starts about how "everything is connected to everything."
If patients have pain associated with the bunion, they typically have seen a podiatrist or orthopedic foot specialist who had some opinion about it. Some are even waiting for surgery.
Why Should Chiropractors Care About Bunions? The Kinetic Chain
During my static visual postural evaluation, I have the patient stand with shoes and socks off. I can see early signs of hallux valgus even before bony bumps begin to appear. The big toe starts to crowd the second toe.
Once I point out that the big toe is not straight and has a change in its optimal angle or there is a visible bump on the big-toe joint, I get them thinking about the linkages within the body. While I'm at it, it's also easy for me to lift the big toe headward and feel for decreased movement of the big toe or foot.
I often see hallux valgus bilaterally, with one big toe having a larger angle than the other. Sometimes the bunion is only noticeable on one foot.
Potential Causes to Consider (From a Chiropractic Perspective)
My current thinking about the cause of a bunion is similar to that of Ron Hruska, from the Postural Restoration Institute (PRI). If someone has a lumbopelvic hip dysfunction and altered gait pattern, he/she is spending a fraction of a second actively balancing on the dysfunctional leg and establishing a supinated foot (let's use the right as example).
This pattern may make it difficult to push off with the right big toe because the patient is unable to get to the left, and pushes off instead with the first metatarsal head. The consequence? The big toe is pushed into an abducted position (bunion).
I often see inhibited gluteals on the right and the patient ends up overusing the gastroc/soleus complex and posterior tibialis muscles for push-off, which creates a supinated position of the right foot.
Part of the overall treatment includes teaching the patient how to fire the right glute and manually balance the pelvis. The left foot may be in a state of passive pronation. The big toe goes into abduction to push to the right in a state of eversion. The patient will typically get heel strike on the right, but on the left you will see heel strike, arch and toe-off (passive).
In the above example, whatever pushes the body to the right (oftentimes some dysfunction higher up in the body) for that fraction of a second while walking or standing causes the big toe to push against the toe next to it. Over time, the bunion forms.
Sometimes, the skin over the bunion becomes tender, red and sore, indicating an acute or chronic inflammatory process that may trigger new bone growth and development of a bone spur. If that happens, a bunion may consist of both soft tissue and a hard bone spur. Painful bunions can produce altered gait, altered standing, and even be uncomfortable while sitting. Insist that patients get their shoes right.
Conservative Care Recommendations
Avoid wearing tight shoes, especially high heels with pointy toes. Buy footwear that is wide in the toe box area.
Shoe pads are an option, especially if they offer relief.
Awareness exercises: "Always try to straighten the big toe." I have patients press the big toe into the floor, and slide the other four toes and foot laterally until the big toe is as straight as possible. This is how I want them to stand all the time.
Stretch the feet and calves. I have yet to meet a patient with bunions who does not have tight calves. I have my patients stand with the forefoot on a ½ foam roll (3" high) with the heels on the ground for 2 minutes at a time, twice a day. After about two weeks, they are able to stand up straighter while doing this stretch. (Calf tightness can be a cause of low back pain in and of itself, so it is important to take this tightness out of the patient's body.)
Strengthen the involved-side glutes, giving the hamstrings length and strength, and the peroneus longus strength up to normal. This allows the first metatarsal to resist the medially directed component of forces associated with hallux plantarflexion.
Use toe spreaders or a bunion splint, especially while sleeping.
Massage CBD serum into the bunion area two to three times a day.
Shockwave (aka pulse wave) therapy. I do this directly over the bunion area. I have found this is an effective way to reduce bunion discomfort and even reduce the deformity itself. I start the treatment at 14 Hz at about 1.4 intensity (and titrate up to patient tolerance of a 6/10 pain score) with the ceramic head on the applicator. I try to deliver 2,000-3,000 pulses per session once a week up to six sessions.
Other Recommendations
Watch your weight: Remember, the rest of the body is pressing down on your feet when you stand, walk or run.
Kinesiology taping: I bring the big toe into a straight position and tape the toe. I teach patients how to do this at home.
Cover the bunion with a cushioning, protective moleskin or gel-filled pad.
Check footwear; offer off-the-shelf shoe inserts or custom-made orthotics.
For the acute flare-up: warm foot soaks, ice packs, whirlpool, more CBD serum, etc.
Have I seen permanent results with conservative therapy? Yes! My best tips and best results have been teaching the patient awareness exercises, home taping of the big toe in a corrected position, shockwave or pulsed therapy and calf stretches.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.