Bad for the Back! Exercises That Can Prevent Healing
Marc Heller, DC
The questions "Who gets well? Who doesn't? Why?" prompted the following observations based on my close to 40 years of chiropractic practice. These observations are limited to a subset of patients who represent probably 40-50 percent of lower back patients with a discogenic or flexion-intolerant lower back. These patients may have sciatica. More often, they just have lower back (and possibly buttock) pain.
For you, the doctor, the first step is to know how to identify these patients. Is this condition on your radar? Do you know how to assess for this problem? If this is unfamiliar to you, read my 2014 article on this topic as a starting point.1 Stu McGill, Craig Liebenson and Phillip Snell have all written and taught extensively on this topic.
"Addition by Subtraction"
For this article, let's focus on the daily activities and exercises of the patient. Over the years, I've learned that people often create or reinforce pain in their bodies by performing incorrect and potentially harmful exercises and daily movements. Stuart McGill strongly emphasizes this point. He says that you first have to eliminate the cause – faulty movement – in order to heal. For the lower back, a patient with disc or flexion-intolerant indicators needs to avoid forward-bending exercise in the early stages of healing.
I call this approach "addition by subtraction": what is taken away often adds immeasurable benefit. I often find this is the most important exercise instruction I can give the patient. I'll never forget the 40-year-old male patient who had a lifting injury and discogenic indicators. Six months later, after seeing another chiropractor and occupational health practitioner, he was no better. What kept him from healing? He would get up in the morning, bend forward and wrap his hands around his ankles. When he stopped doing this, he finally started to improve.
What Exercises Need to Be Avoided?
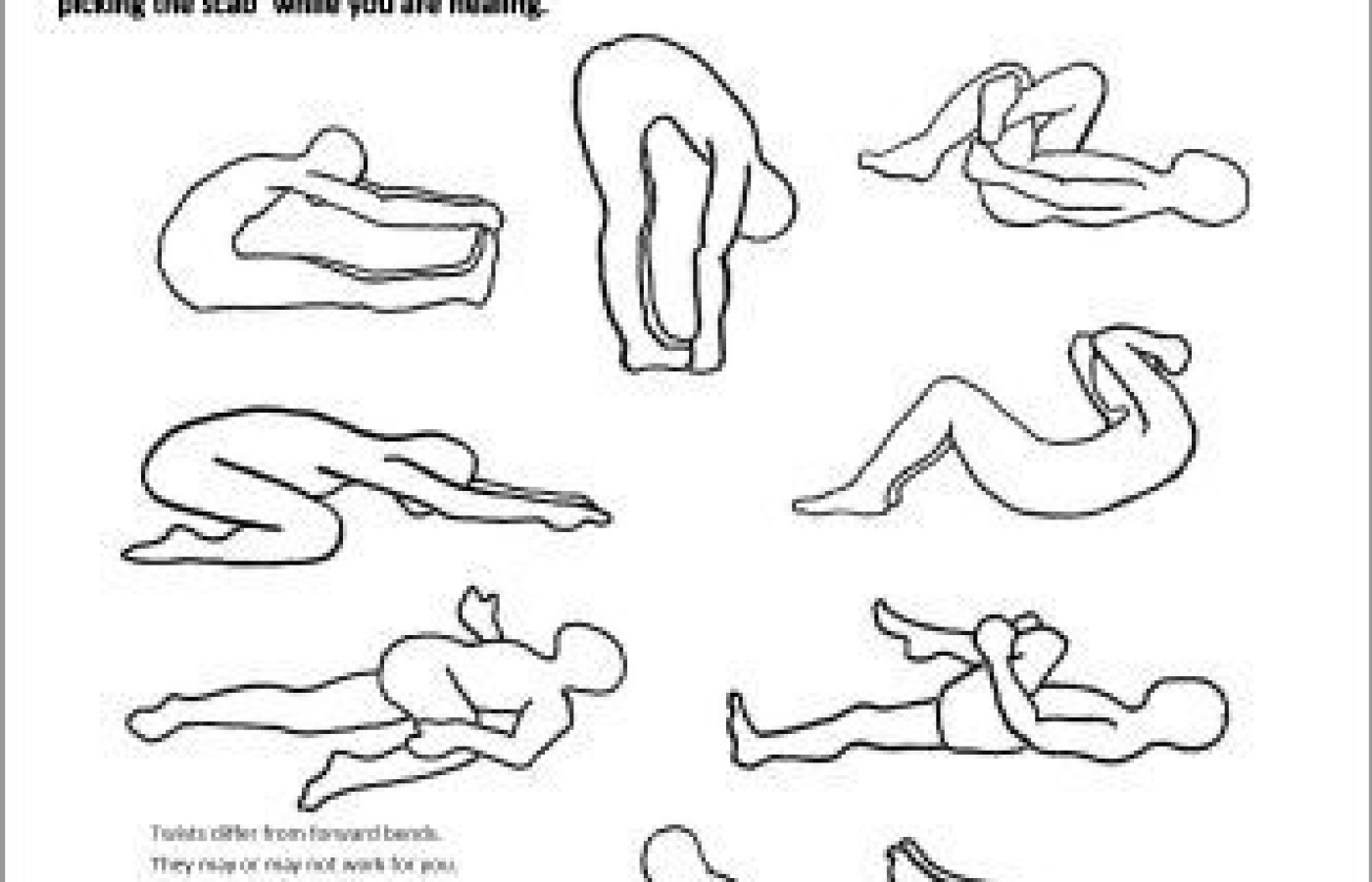
I've created a handout illustrating these potentially risky exercises. I am happy to share this handout with you. Please share freely, both with your patients and your colleagues (and please attribute). I've titled it, "Exercises to Avoid!" I want the patient to pay attention and stop doing these movements for now.
Click here to download handout
I've already told these patients to avoid flexion exercises, crunches and toe touches. In spite of this instruction, an unbelievably high percentage of my patients look at this sheet, point at a couple of the contraindicated exercises and say, "Oh, I do that one all the time." These simple pictures seem to get the message across more powerfully.
The conundrum / counterintuitive part: Most of these exercises will not cause immediate pain unless there is pronounced inflammation. The usual effect of forward stretches is temporary relief. The forward stretches are quieting the sensors within the lumbar extensors. The aggravation, the worsening of the patient's pain, usually shows up 20 minutes to an hour later. This response can be quite confusing to the patient.
Yes, it is possible that your patient can develop fear of flexion. This can become a problem, usually months down the line, when it is time for them to expand their movement repertoire. First, they have to quiet the sensitized area, and stopping flexion is critical at this early stage. "Early stage" does not necessarily mean they hurt themselves one week ago. Discs can remain irritated for years or decades if they are continually aggravated and reinjured. The patient needs to "quit picking the scab."
Putting Safe Movement Into Practice
By the way, these same principles of safe movement strategies apply to daily activities as well. Do your patients know how to safely get up from and sit down in a chair? Do they know the best way to tie their shoes? Are they slouching while sitting or looking at their phone?
Simple actions performed incorrectly over and over can have profound repercussions. I repeat: Your patients cannot get well if they are continually re-injuring themselves. These patients need to learn to bend forward safely, activating the correct muscles while maintaining lumbar neutral. The hip-hinging principle, using the large buttock muscles instead of the smaller lumbar extensors, is absolutely critical for these patients. For some patients, this is easy to learn; for others, it is quite difficult. For just about everyone, it requires a newfound awareness in many everyday movements.
What about lifestyle? There are plenty of lifestyle challenges in getting healthy, but here is one that strongly impacts the flexion-intolerant lower back: too much sitting! Sitting is flexion. (I appreciate the statement, "Sitting is the new smoking," even if it is an exaggeration.) If required to sit at work, are your patients taking sufficient movement and standing breaks? They need to counteract the effects of being in a flexed position for long periods of time.
What about attitude? Is your patient afraid to move or exercise for fear they will hurt themselves? So many people in pain are hesitant to exercise. This contributes to the deconditioning that is so common in chronic pain.
Of course, pacing is critical. What can your patient do? On the first visit, I make it a point to find and prescribe at least one exercise that relieves pain. I want the patient to experience success with something they can do for themselves. This is such a critical step. An empowered patient moves more easily through fear into healing.
Reference
Heller M, Snell P. "Flexion-Intolerant Lower Back Pain (Pt. 1): Diagnosis." Dynamic Chiropractic, Jan. 15, 2014.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.