Editor's Note: This article is adapted from Dr. Morgan's 2015 book, Hero Workouts.
Cross-fitness centers are expanding in number and increasing in popularity. To remain relevant to this growing portion of society, practitioners need to learn about the exercises and injuries common to this group.
I have a love-hate relationship with cross-fitness. I love the functional aspect of cross-fitness workouts and the push toward functional motion patterns, versus the use of weight-lifting machines and muscle isolation exercises. Additionally, I like the metabolic aspect of cross-fitness workouts, which can have profound effect on athleticism and performance.
On the other hand, what I don't like about cross-fitness is the lack of uniformity in the qualifications of cross-fitness instructors and the timing of certain exercises, like heavy deadlifts for time or 30 snatches for time, after an athlete is already fatigued and prone to injury.
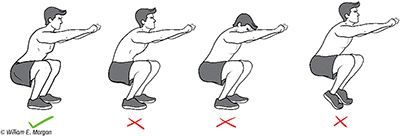
FIG 1 Before progressing to certain exercises such as squatting or the clean and jerk, athletes should be screened with an exam which includes squatting. A properly executed squat should include (1) an arch in the lower back, (2) head up and (3) heels on the ground and the shins near to perpendicular to the ground.
There is also a wide range of expertise when it comes to the people who train clients in these functional gyms. Some of the athletic trainers are fantastic. Some boxes (cross-fitness lingo for a cross-fitness gym) are run by chiropractors or physical therapists, or at least have chiropractors as clients or consultants. In my opinion these tend to be more prone to adapt exercise programs to individuals to avoid injuries. Unfortunately, there are also trainers who are not as knowledgeable in adapting fitness programs to the needs of an individual. (But to be fair, the same can be said about fitness trainers in any gym.)
Certainly cross-fitness has disrupted a well-entrenched fitness industry by capitalizing on people's desire to develop social bonds, compete and get into really good shape. In several ways, cross-fitness is more of a sport than a fitness program. Although many doctors feel these programs are injuring their patients, I believe it is a good idea to make peace and communicate the particular needs of our patients. The cross-fitness movement is adapting and evolving, albeit slowly, improving the programs and reducing the risk of injury.
Cross-fitness, as the name implies, combines a cross of various fitness methods to develop athletic prowess. Included in the program are Olympic lifts, gymnastics, kettlebells, plyometrics, calisthenics, running, swimming, rope climbing and mobility exercises. Certainly there would be a concern if a patient with a hypermobility syndrome such as Ehlers-Danlos began performing dips, push-ups or muscle-ups on gymnastic rings. These exercises could lead to a dislocated shoulder. Equally distressing is the thought of a lumbar disc patient performing heavy deadlifts in a timed event.
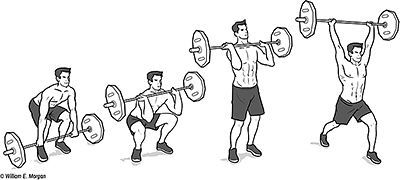
FIG 2 The clean and jerk is a technical lift, which I feel is best performed with one or two repetitions at a time. Since this lift requires speed, timing and power, it should not be done with high repetitions or when fatigued.
Some people should never do particular exercises, but some exercises should not be done by anyone. Let's address Olympic lifting, squatting motions, and the importance of thoracic spine motion during overhead lifting.
Olympic Lifting
Successful Olympic weight-lifters have unique body types. Not everyone has the genetics to be a successful and safe Olympic weight-lifter. The combination of hip-joint, thoracic-spine, foot / ankle and shoulder mobility must be coupled with shoulder stability and power.
Those with more shallow hip sockets will have a greater range of hip motion, and are genetically better suited for performing Olympic lifts and squatting motions. Those with deep, more stable hip joints are no less capable athletes, but they probably won't be great Olympic lifters or proficient at performing deep squats.
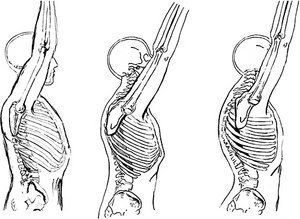
FIG 3 A normal, flexible spine will allow normal shoulder motion during overhead activities (left). Reduced spinal motion will impede normal shoulder motion (center). Forcing the shoulder overhead, even though impeded by an increased kyphosis or loss of spinal motion, will result in shoulder impingement.
By having patients perform a few squats in your office, you can get a good idea of whether or not they should progress to performing an Olympic lift such as a clean and jerk or a snatch. The patient's feet should be slightly wider than shoulder-width apart and the toes slightly turned outward. The patient should be able to maintain a lumbar lordosis throughout the squat. The head should be up (not flexed or excessively extended), and the heels should remain on the ground.
If there are flaws in squatting patterns, they should be addressed before this patient can progress to an exercise such as the clean and jerk. Mobility exercises for the hip, the spine or the foot can be used to isolate the source of the motion flaw. Chiropractic adjustments to the spine, hip, and foot may be indicated.
The Clean and Jerk
Proper technique is imperative when performing the clean and jerk, and proper technique requires coaching. While not everyone has the genetics to perform the clean and jerk to high levels of performance, most athletes should be able to perform this exercise even if they must modify their technique or perform this exercise with kettlebells.
The Aggregate of Thoracic Spine-Shoulder Motion in Overhead Lifting
Thoracic spine motion is required for all end-range shoulder motions. End-range shoulder motions include overhead pressing, the clean and jerk, pull-ups, handstands and other overhead lifts. If the thoracic spine lacks significant motion, there is a much greater likelihood of shoulder impairment.
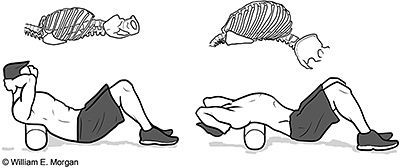
FIG 4 Those lacking sufficient thoracic spine motion will have impeded shoulder function. In addition to chiropractic manipulations to the thoracic spine, the use of a foam roller can enhance thoracic spine mobility, which in turn will improve shoulder motion and function. This schematic shows the effect of a foam roller in mobilizing the thoracic spine and opening the chest wall.
Shoulder injuries are particularly prevalent when performing exercises such as kipping pull-ups and the overhead snatch. Loss of thoracic motion or a hunched upper back (increased kyphosis) can be treated with adjustments and by rolling the thoracic spine over a foam roller or gym ball.
Thoracic Adjustments for Reducing Shoulder Pain
Thoracic adjustments might be the simplest answer to reducing pain in an impinged shoulder. In a 2009 study by Strunce and colleagues, a thoracic spinal manipulative thrust was performed on a sample of 56 individuals with symptomatic shoulders from impingement. After two days, there was a significant decrease in pain levels in more than 50 percent of individuals.
The cross-fitness emphasis on pull-ups and overhead lifting may produce a glut of shoulder injuries from otherwise dormant thoracic and shoulder impairments. By recognizing the functional relationship between the thoracic spine and the shoulder joints, we can help athletes remain active and pain-free as they engage in their preferred activities.
Resources
Myer GD, Kushner AM, Brent JL, Schoenfeld BJ, et al. The back squat: a proposed assessment of functional deficits and technical factors that limit performance. Strength & Conditioning J, Dec 2014;36(6):4-27.
Borstad JD, Ludewig PM. The effect of long versus short pectoralis minor resting length on scapular kinematics in healthy individuals. J Orthopedic Sports Physical Therapy, 2005;4:227-238.
Codman EA. The Shoulder; Rupture of the Supraspinatus Tendon and Other Lesions in or About the Subacromial Bursa. Boston: Thomas Todd, 1934.
Crawford HJ, Jull GA. The influence of thoracic posture and movement on range of arm elevation. Physiotherapy Theory and Practice, 1993;9:143-148.
Crosbie J, Kilbreath SL, Hollmann L, York S. Scapulohumeral rhythm and associated spinal motion. Clinical Biomechanics, 2008;23:184-192.
Greenfield B, et al. Posture in patients with shoulder overuse injuries and healthy individuals. J Orthopedic Sports Physical Therapy, 1995;5:287-295.
Kibler BW. The role of the scapula in athletic shoulder function. American J Sports Med, 1998;26:325-337.
McClure PW, Michener LA, Sennett BJ, Karduna AR. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder and Elbow Surg, 2001;10:269-277.
Stewart S, Jull GA, Ng, JKF, Willems JM. An initial analysis of thoracic spine movement during unilateral arm elevation. J Manual & Manipulative Therapy, 1995;3:15-20.
Strunce J, et al. The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoulder pain. J Manual & Manipulative Therapy, 2009;17:230-236.
Theodoridis D, Ruston S. The effect of shoulder movements on thoracic spine 3D motion. Clinical Biomechanics, 2002;17:418-421.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.