Chiropractic Management of Lower Extremity Disorders
The Hallux Joint and Athletic Power (Part 1)
William E. Morgan, DC
Editor's note: This is part 1 of a two-part article on hallux joint dysfunction and chiropractic treatment strategies. Both parts are the initial installments in an ongoing series on chiropractic management of lower extremity disorders.
The importance of normal motion of the great toe (hallux) cannot be overstated. The motion of the great toe into dorsiflexion is extremely important to normal, pain-free gait and to transferring power in running and athletics. The great toe is unique among the phalanges, metatarsals and tarsals for its contribution to optimized foot stiffness in the propulsion portion of gait.
The Importance of First MPI Dorsiflexion
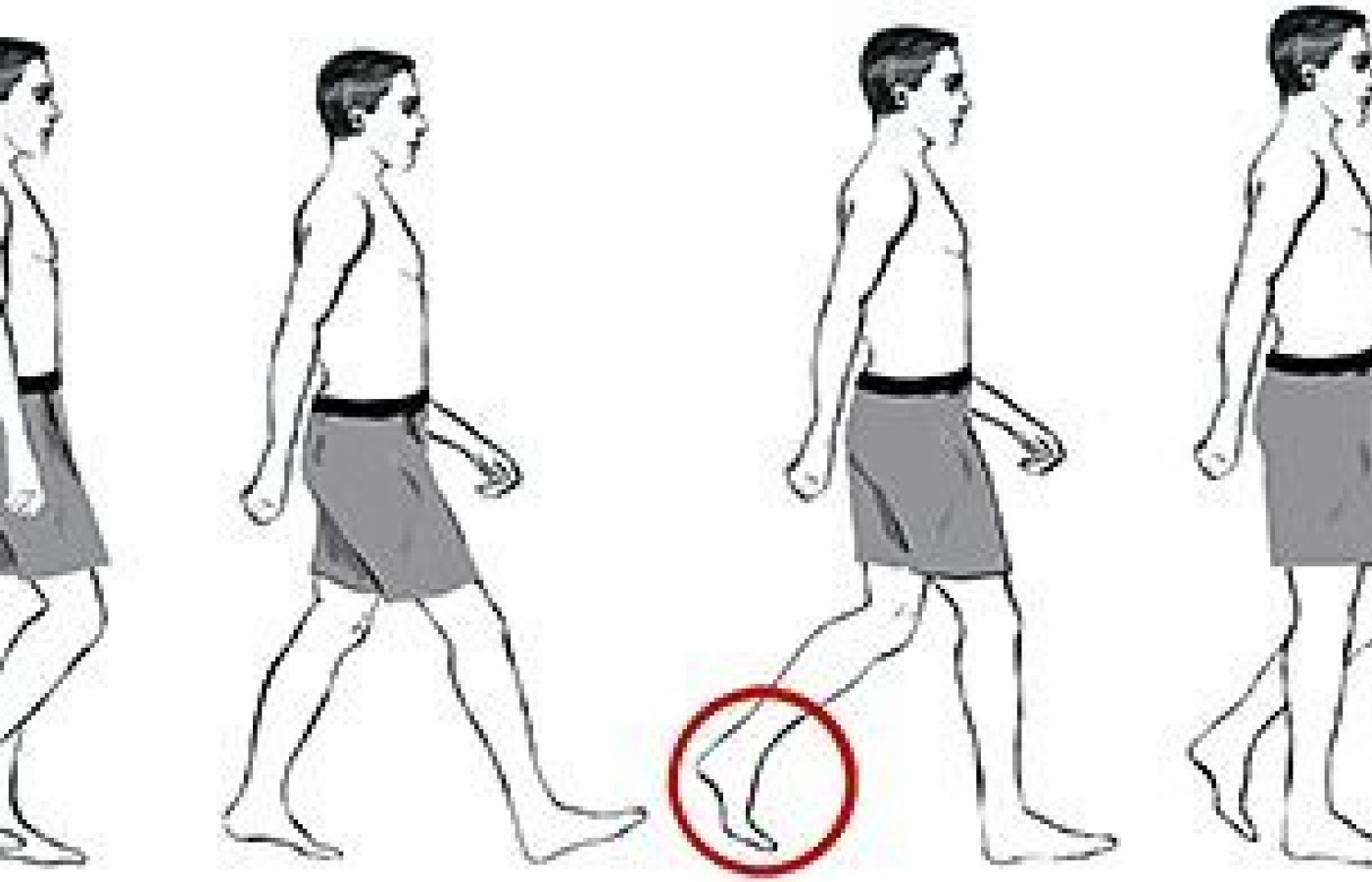
The first metatarsophalangeal joint (MPJ) has a distinctive significance beyond its size, and this joint's ability to dorsiflex is important in the ability to propel us forward with efficiency and speed. Paradoxically, significant motion (dorsiflexion of 65 degrees or more) of the great toe is required for optimized stiffness of the midfoot during the propulsion phase (toe-off) of the gait cycle. (Figure 1) Dorsiflexion of the hallux is paramount in maximizing the "windlass" effect for leveraging stiffness and strength in the foot.
The Windlass Mechanism
Figure 1: The gait cycle. The fourth figure from the left shows the left foot during the propulsion phase of gait. It is important that the hallux (great toe) is able to adequately dorsiflex during the propulsion phase of the gait cycle to increase foot stiffness and maximize power transfer.
A windlass is a simple machine used to lift heavy loads. Through the use of pulleys, ropes and cranks, a windlass magnifies the load-lifting capacity of the operator. The foot has a mechanism that operates much like a windlass pulley system, and this mechanism magnifies the strength of the foot in propulsion during gait.
In the foot, the windlass effect results from the combined forces of the extrinsic muscles (gastrocnemius, soleus and tibialis posterior), intrinsic foot muscles, and the tension enhancement created by dorsiflexion of the great toe. This effect is further enhanced by the sesamoid bones functioning as pulleys.
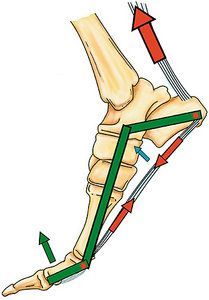
This windless effect increases arch height, plantar fascia tautness and foot stiffness. This allows for an efficient transfer of power and propulsion during the toe-off phase of the gait cycle. Without optimal foot stiffness during the propulsion phase, the midfoot is slackened and less efficient in transferring force. (Figure 2)
Figure 2: The windlass effect magnifies the power of the foot, particularly with dorsiflexion of the first toe, which adds tension and raises the arch.
If the hallux is unable to fully dorsiflex, the foot will not be as stiff during the propulsion phase of gait; this results in pushing off of a slackened (versus rigid) foot. Pushing off of a slackened foot will result in loss of propulsive efficiency and power. This reduces efficiency of gait.
This power drain will need to be made up for high in the kinetic chain, which can lead to injuries higher in the chain, such as the knee, hip, sacroiliac or lumbar spine.
Dizzy Dean's Toe Injury
The importance of the hallux in the global kinetic chain of body is epitomized in the career-ending story of the baseball pitching great, Dizzy Dean, who pitched the 1937 all-star game with a broken toe. His pitching biomechanics were so dramatically altered by the toe injury that by the end of the game, his pitching shoulder was irreparably damaged, forcing him into early retirement. A broken toe resulted in a ruined pitching shoulder.
A dysfunctional hallux can set the stage for injuries throughout the kinetic chain from the foot to the knee, hip, lower back, and even to the shoulder. I am still surprised by the common responses of patients after I've adjusted a fixated hallux: "Doc, I am squatting so much better since you adjusted my toe" or "My knee pain is better." I even have patients with persistent shoulder complaints recover after I've adjusted the foot and ankle.
Hallux Disorders
Turf toe is a first metatarsophalangeal injury commonly attributed to playing on artificial turf. It occurs when the ligaments and cartilage of the great toe are damaged. The term is closely associated with football and the forceful driving off of the great toe and jamming of the great toe during play. However, this injury can also affect athletes in other sports, including baseball players, soccer players, wrestlers, gymnasts and dancers.
One common mechanism of injury in American football may occur when a player's toe is extended and fixed on the ground, and another player lands on the back of their calf. Turf toe can progress and lead to chronic pain, stiffness and progressive degeneration.
Hallux limitus is the diagnosis of a stiffened great toe (big toe). As the name implies, it is characterized by reduced motion of the great toe at the first metatarsophalangeal joint. Hallux limitus may also be characterized by pain and may progress to the more debilitating arthritic condition known as hallux rigidus (a painful, rigid degeneration of the metatarsophalangeal joint).
The hallux limitus may be pain free and not recognized until symptoms occur and it has progressed toward becoming a hallux rigidus. The normal motion of the MPJ is very important in ambulation. This motion also affects the foot, ankle, knee, hip and even the lumbar spine.
Hallux limitus can be detected by testing range of motion of the toe, particularly dorsiflexion of the MPJ; and by motion palpation of the joint through the various planes of motion: anterior to posterior shear, medial to lateral shear, rotation, and long axis distraction. The normal passive range of motion of the MPJ in dorsiflexion is between 50 degrees and 100 degrees. For optimal forward propulsion, the great toe needs at least 65 percent of dorsiflexion. Note that some authors recommend range of motion be tested by observing the patient's gait versus static range-of-motion testing (static testing in open or closed chain).
Hallux rigidus is a painful, rigid degeneration of the metatarsophalangeal joint that tends to worsen with time, which can result in erosion of hyaline cartilage and subsequent debilitating pain. Hallux rigidus may progress to having an exostosis, creating a bony barrier on the dorsum of the joint. This creates a hard barrier to dorsiflexion of the great toe. It is important to identify and treat hallux limitus before it progresses to hallux rigidus.
Differential Diagnosis
Other conditions of the hallux include those which have varied response to manual treatment. I list them more as differential diagnoses, rather than a list of conditions that will respond to adjustments. These conditions include hallux valgus (bunions), hallux varus, gouty arthritis, rheumatoid arthritis, hammer toes, and claw toes. I do not want to generalize the management recommendations of this article to those conditions.
Causes of Hallux Limitus and Hallux Rigidus
While hallux limitus and hallux rigidus have often been attributed to idiopathic origins, there are also some identifiable causes of these conditions:
Congenital variations in anatomy or genetic predisposition
Occupational stresses (occupations that require kneeling and pressure on the hallux, such as carpet layers or plumbers)
Improper footwear: high heels or improperly fitting shoes
Repetitive stress: ballet dancers, runners, and athletes in general
Overt injury
Prolonged immobilization (casting or surgical boots)
The most common causes of hallux limitus are inherited anatomical variations, such an elongated first metatarsal bone or a shortened second metatarsal. Injury, such as stubbing the toe, jams the articular surfaces together, and if severe enough, can lead to chronic joint stiffness, hallux limitus and possibly hallux rigidus.
Resources
Root ML, Orien WP, Weed JH. Normal and Abnormal Function of the Foot. In: Clinical Biomechanics, Volume II. Clinical Biomechanics Corp. Los Angeles, 1977.
Buell T, Green D, Risser J. Measurement of the first metatarsophalangeal joint range of motion. J Am Pod Med Assoc, 1988;78:439.
Bojsen-Moller F, Lamoreux L. Significance of free dorsiflexion of the toes in walking. Acta Orthop Scand, 1979;50:471.
Hetherington VJ, Johnson RE, Albritton JS. Necessary dorsiflexion of the first metatarsophalangeal joint during gait. J Foot Surg, 1990;29:218.
Nawoczenski DA, Baumhauer JF, Umberger BR. Relationship between clinical measurements and motion of the first metatarsophangeal joint during gait. J Bone Joint Surg, 1999;81(3):370-6.
Part 2 of this article covers chiropractic management of hallux disorders.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.