I am not sure why it has taken me so long, but after 104 articles, I am finally writing about visceral manipulation. Let's begin with some background on how I started studying visceral work. In 1994, I worked in an interdisciplinary clinic, where I got to rub shoulders with a manipulating osteopath. I had always been interested in low-force methods, but this was my first introduction to the osteopathic ways of using low-force manipulation. I was impressed by the osteopathic methods and sought out a way to learn them.
Most PTs who do manual therapy use methods originally developed in osteopathy. Relatively few DOs in the U.S. are primarily manual practitioners, although some certainly are, and they can be very good. DCs generally are not exposed to the osteopathic model unless we search outside of our own profession.
What I like about osteopathic manipulation methods are their subtlety. Muscle energy and counterstrain use minimal force to move joints. The methods depend on patient positioning and in the case of muscle energy, small contractions of the patient's musculature, followed by relaxation while the joint is moved.
Barral and Abdominal Fascia
On to the French, the next set of osteopaths with whom I studied. When I was first exposed to Jean Pierre Barral's work, I was amazed by its precision and gentleness. He seemed to have taken the osteopathic model, applied it to additional tissues, and made it something more; perhaps more comprehensive, certainly more three-dimensional.
Barral is a fascinating character. DOs in France before 2009 (and chiropractors as well) were not licensed. Yes, they had professional schools and professional organizations, but they were not licensed or regulated by the state. Barral, at least in my view, had a somewhat unique way of developing technique. He was not particularly interested in the literature, or even in what others did or said. He wanted to read primary sources, such as anatomy and physiology, and then listen to the body.
He developed his own methods, you could say in a vacuum. I have observed others who've taken this lonely path; Judith Aston of Aston patterning comes to mind. This path can lead to brilliant observations and things that no one else sees, but can easily lead one astray as well.
Barral applied his amazing palpation and listening skills to the abdomen. He deeply studied the anatomy of the fascia, looking at the fascia that supported the abdominal organs, how fascial tension patterns affect organs and their relationships in the abdomen.
The visceral manipulation work brings a depth of study to applied anatomy. Other manual therapy clinicians and systems have certainly done some sort of visceral manipulation. In applied kinesiology, working on hiatal hernias and the ileocecal valve is common. Barral brought a subtlety and a completeness to this work.
Instead of just looking the ileocecal valve, the right lower abdomen includes the cecum, the ascending colon, the right ovary, the right kidneys, and even the renal arteries as they feed the kidneys. All of these are visceral structures that could lose normal mobility and thus be addressed with manipulation. All of these structures could pull on other structures, and thus affect function, in the tensegrity type of model applied within visceral manipulation.
Visceral Manipulation Basics
Visceral manipulation is different from many of the reflex systems that attempt to affect organs. The practitioner is not pressing on a distant reflex point, such as a neurolymphatic, hoping to improve lymphatic drainage. The practitioner is directly working on the fascia surrounding the organ, hoping to improve mobility. This is quite similar to many other fascial models used in various forms of bodywork.
I spent many years studying with Barral and the other visceral teachers in his group. As a chiropractor, I mostly use these techniques on musculoskeletal pain that is not resolving using the other tools in my toolbox. I have solved many knee pain cases by lifting the kidney. I have helped long-standing thoracic or rib-cage pain by releasing the gastroesophageal junction on the left, or the whole gallbladder, liver, bile duct, and sphincter of the Oddi complex on the right.
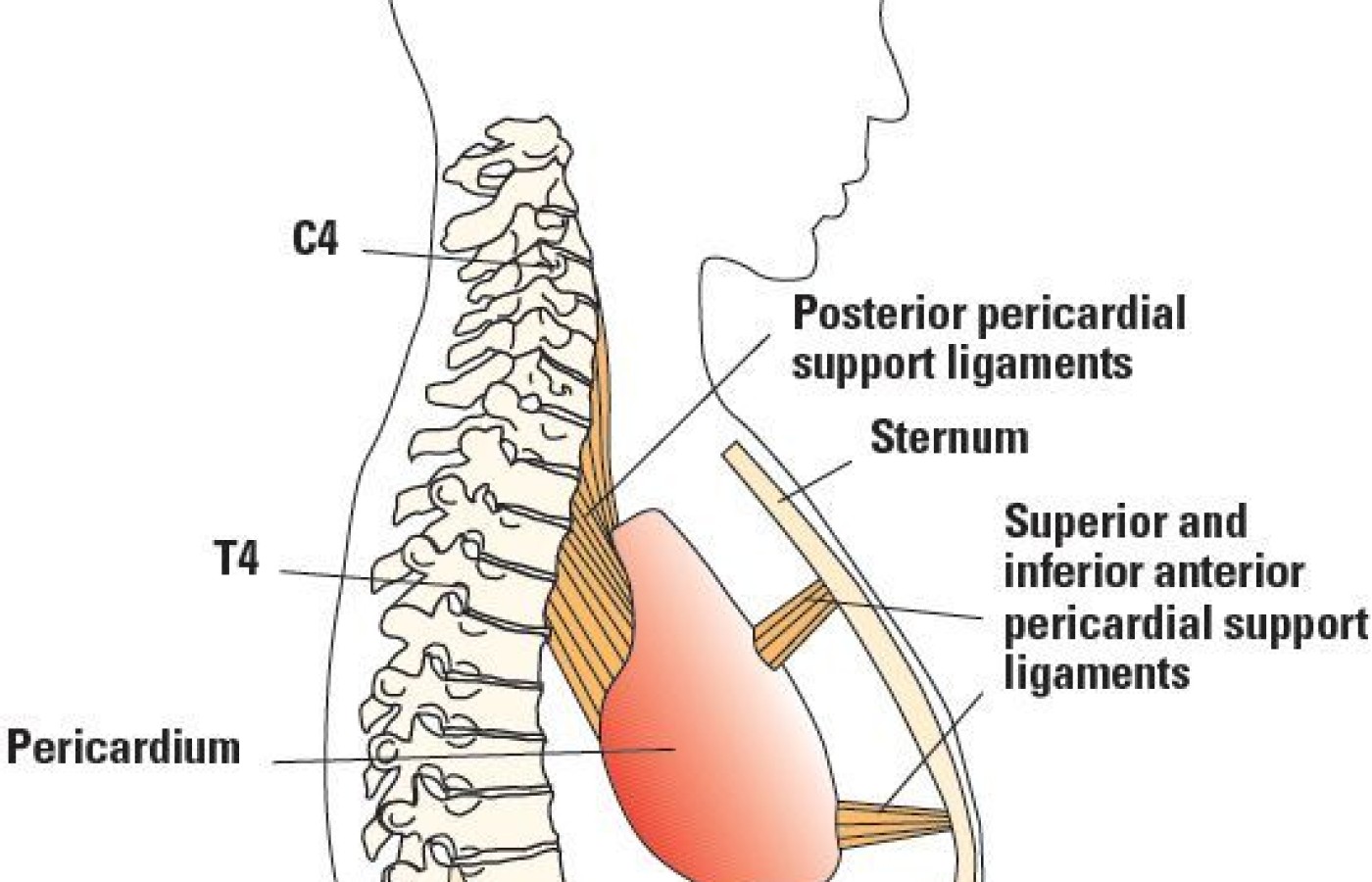
Figure 1: The pericardium and its support ligaments, connecting to the cervical and thoracic spine and sternum. The pericardium is suspended posteriorly by a continuous skein of ligament from the bodies of all vertebrae C4-T4, and anteriorly to the posterior surface of the sternum by two ligamentous local thickenings of the mediastinum at the levels of the third and fifth ribs. Pericardial support ligament strains produced by whiplash or other impact injuries are frequently expressed as low cervical and upper thoracic stiffness and pain. Reprinted with permission from Jeffrey Burch, MS.
Visceral manipulation has a deep grounding in anatomy, with study of the fascial linings of the organs. Another quality of visceral manipulation is the touch; the subtle three-dimensional way of working with the visceral fascia. This is really hard to describe in words. This work is definitely within the tonal or subtle type of myofascial work. Barral's "listening," the concept of just putting your hand on the body and feeling where you are pulled toward, has strongly influenced my overall practice, not just my visceral work. One of the main myofascial techniques I use and teach, which I have named engage, listen, follow, is my interpretation of the way Barral releases fascial tissues.
Barral has expanded his work further, with a method aimed at nerves (neural manipulation), using the same principles to apply his unique manual therapy approach directly to the fascial layers on the outside of the nerves. His text on this is Manual Therapy for the Peripheral Nerves.1
Barral is a prolific author, with at least nine books to his credit. Besides Visceral Manipulation, his first book, another of interest to chiropractors is Trauma, An Osteopathic Approach. Barral outlines how the solid organs get thrown around in trauma, as they are heavy and fluid filled, and have inertia, and then can cause problems down the line.
How many of us check the liver when the rib cage has been injured? How many of us look at the kidneys in any kind of lower back or lower extremity problem? Barral's trauma text also gave me a deeper understanding of the dura mater and how cranial manipulation works.
What about the evidence? As usual in systems of manual techniques, the evidence is sparse. I am afraid I could repeat this statement about almost any manual technique. You might differ with me about "your" favorite technique, but the reality is that the depth of evidence about the things we do is exceedingly thin. (My next article will take a look at the evidence for manual therapy and chiropractic in general.) I have seen very little hard evidence for the efficacy or utility of visceral manipulation.
Barral's site, at the Barral Institute, has a page on research, but the actual peer-reviewed studies on visceral manipulation are minimal. I have linked to the research page here.2 I include a link here to one of the few real studies done on visceral manipulation, on mobility of the kidneys, elegantly done and confirmed using ultrasound, I am not clear on where it was published,3 although the paper was presented at the 3rd International Fascia Research Congress, April 2012, in Vancouver, British Columbia.4
I think it is valid to ask whether a method has biological plausibility; does it make sense with what we know about anatomy and physiology? Personally, I put visceral manipulation in the same category as most of the techniques we use – useful for the right patient at the right time. I also appreciate Barral for raising the bar; for expanding our view of the body.
Another question; Can we check our results using the technique outside of the internal system? For example, when someone is limping, tender in the medial joint line of the knee, and has limitations of range of motion in the hip or knee, and I think I need to lift the kidney as a treatment, how should I reassess them? It is not enough to palpate and say that the kidney is now moving better. Your knee should feel better.
I want evidence, in the moment, to assess whether their knee is better. I should watch the patient walk, recheck my tender point and recheck ROM. Are these functional tests different and improved? If so, my mini clinical trial of visceral for that knee has a reasonable chance of success. It is obviously harder to determine if kidney function has actually improved.
A Few Clinical Examples
When I write about technique, I usually try to give you some practical thing to try out. I am not going to attempt that in this article. Visceral manipulation does require hands-on training. So, I will tell a couple of personal stories about visceral manipulation instead. In nearly every patient who either has a tendency toward gallbladder issues or has had their gallbladder removed, there are potential visceral restrictions all through the bile tract. This would include the liver, the gallbladder, the bile duct (which takes the bile toward the intestine), and the sphincter of Oddi (or common bile duct, where the pancreatic fluids and bile duct fluids both are expelled into the small intestine).
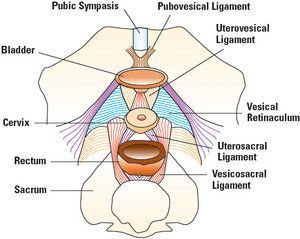
Figure 2: The suspensory ligaments of the pelvic organs. Note the connections between the pubic symphysis, the bladder, the uterus and the sacrum. The pelvic organs are attached by a system of ligaments to the pelvic bones and sacrum. Asymmetrical tensions in these ligaments will produce pelvic and sacral misalignment. Reprinted with permission from Jeffrey Burch, MS.
One of the principles of visceral manipulation is that sphincters can become dysfunctional, and that we can test and correct this. Correcting the congestion along this whole line has been profound for abdominal issues related to bile or the gallbladder, as well as for rib-cage and thoracic pain.
Here is another example. When the patient has sacral or SI problems that do not resolve, what else can be pulling on these structures? Besides the lumbar spine, hips,and the rest of the lower extremities, do you even think about the structures anterior to the sacrum? There is a whole set of visceral ligaments (remember, visceral ligaments are much less thick and strong than joint ligaments) connecting from the pubic symphysis directly posterior, encircling the bladder, the uterus in females, and the rectum. If you buy the visceral model, you can see that these structures could pull on the sacrum.
The pericardium is another fascinating visceral structure. The pericardium is the sac of the heart, and the illustration above shows its connection to the lower neck and upper thoracic, and to the sternum. You have to suspend your disbelief a bit to imagine being able to palpate and move the pericardium through the anterior chest structures. After doing this many hundreds of times, I am reasonably confident that I can tell a qualitatively different feeling of sternal or sternochondral restrictions versus pericardial restrictions.
If you are competent at visceral manipulation, the pericardium is one of the visceral structures you would check for persistent neck or upper back pain. The pericardium is another of the dense, fluid-filled structures that can get thrown around in trauma.
I hope I have stimulated your curiosity about visceral manipulation. I experience the body, the fascia and the tissues I can work on as much more three-dimensional by including the viscera in the field of view. As usual, I have taken a huge subject and tried to give you a brief overview. The Barral Institute site has more information, and others also teach various variations on visceral work.
References
Barral J-P, Croibier A. Manual Therapy for the Peripheral Nerves. Elsevier Ltd., 2007.
Michallet J-M. "Kidney Mobilization and Ultrasound Documentation."
Tozzi P, Bongiorno D, Vitturini C. "Low Back Pain and Kidney Mobility: Local Osteopathic Fascial Manipulation Decreases Pain Perception and Improves Renal Mobility." Presented at the 3rd International Fascial Research Congress, Vancouver, B.C., April 2012.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.