The Iliopsoas: A Possible Cause of Acetabular Labrum Tear
Warren Hammer, MS, DC, DABCO
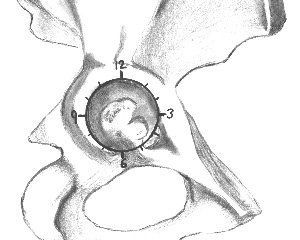
An anatomic study that appeared recently in the American Journal of Sports Medicine1 identified - for the first time - the cross-sectional anatomy of the iliopsoas tendon at the level of the labrum. Several authors have implicated iliopsoas impingement on the anterior labrum as a cause of labral tears. They have stated that a tight iliopsoas tendon could cause compression over the anterior capsulolabral complex, leading to labral lesions. Labral tears at the 2 o'clock to 3 o'clock position of the acetabulum (see image below) are directly under the iliopsoas tendon. This labral tear is considered an anterior tear, while most labral tears caused by trauma, femoroacetabular impingement, capsular laxity/hip mobility, dysplasia or degeneration are usually found at the 11:30 to 1 o'clock position.
The hip labrum is important because it maintains joint congruity, acts as a sealant to the hip joint, and maintains negative intra-articular pressure that stabilizes the hip joint.1-2Surgeons have noted tight psoas tendons overlying and impinging on torn or inflamed anterior labrums.3 Ninety-two percent of labral lesions are in the anterior quadrant of the acetabulum and are related to degenerated hips.1
Labral tears at the 2 o’clock to 3 o’clock position of the acetabulum are directly under the iliopsoas tendon.
The above information is important since tightness of the iliopsoas should become a routine evaluation not only for hip patient complaints, but also as a preventative measure against hip pain and possible eventual degeneration. In a previous article,4 I discussed how a tight psoas can also be responsible for compressing the hip capsule. Tightness of the hip capsule can create an increase in the intra-articular pressure. High pressure within the hip capsule creates high intraosseous venous pressure due to blockage of flow in the periarticular veins, such that hemodynamic changes in the bone marrow are secondary to high pressure within the capsule.5
The iliopsoascan be stretchedby methods such as post-facilitation stretching, fascial release, and active isolated stretching6(also discussed previously); friction massage or Graston Technique at the insertion on the lesser trochanter can also be beneficial. Treating the psoas also requires evaluation and treatment of hip mobility. Loss of hip motion can be directly related to restricted myofascia, and restricted fascia could be due to loss of joint motion. Both must be considered. Reflex inhibition of tight myofascia can be responsible for a tight hip capsule, rather than capsular contraction.
Ferguson7 states that to create absolute lengthening of the psoas, it is necessary to normalize femoral/acetabular dysfunction (F/A), just as normal F/A function will depend on a fully lengthened psoas. Hip joint-play dysfunction should be evaluated. There will never be normal joint function if myofascial dysfunction abnormally stresses the joint, nor can there be normal myofascial function if there is joint dysfunction. Normal muscle length requires normal joint function.4
Patients with labral tears usually complain of groin pain, a clicking hip, sharp, catching pain and popping. Sometimes the pain may be localized to the anterior groin, just proximal to the trochanter, or deep within the buttock.7 The hip symptoms may be subtle, such as a dull activity-related or positional pain that just does not seem to improve. I have treated patients with these types of symptoms and some of them definitely had shortened iliopsoas muscles. One was diagnosed with iliopsoas tendinosis and labral tearing that responded to manual therapy over the insertional tendinosis area.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.