That painful clicking shoulder, especially in a thrower, could be a torn labrum usually referred to as a superior labral tear that is anterior to posterior in direction (SLAP) between the 10 and 2 o'clock position of the glenoid. The labrum is located at the circumference of the glenoid cavity and is the attachment point of the shoulder capsule. Anchoring of the capsule to the glenoid labral rim is important for glenohumeral stability.1 Tearing of the labrum, which is attached to the glenoid, is an indicator that the capsule also is not attached at that location. There are four main types of SLAP lesions with the most common being the type 2, the only type where there is an actual detachment of both the labrum and biceps that inserts into the labrum.1
Physical examination for a shoulder labral tear is equivocal and it's disheartening to realize that most of the labral tests are not very sensitive or specific. Tests such as O'Brien, the crank test, Speed test, anterior slide, the compression-rotation test, biceps load and Yergason test are no longer considered predictive for SLAP lesions,1,2 even when they reproduce a painful click. Kibler1 stated that no single test is diagnostic and recommended at least five tests before making a decision. When the O'Brien test was first presented, O'Brien reported that his test was 100 percent sensitive and 98.5 percent specific for labral tears. Guanche, et al.,3 used arthroscopic evaluation before surgery to determine if particular labral tests were as valid as they were supposed to be and found the O'Brien test to be 63 percent sensitive and 73 percent specific.
He found similar results with other tests and concluded that a decision to proceed with surgery should not be based on clinical examination alone.3
Yang-Soo Kim, et al.,2 discovered a new test for superior labral tears of the shoulder. They used what they call the Passive Compression Test (PCT), which was performed independently by two physicians as the first test before any other diagnostic evaluation including MR arthrogram imaging was used. All the lesions were eventually verified by arthroscopic examination and arthroscopic surgeries. Of the 61 shoulders examined, 31 demonstrated a positive PCT and 30 demonstrated a negative test result. Of the 31 patients with a positive test, 27 had confirmed SLAP tears. Of the 30 patients with a negative PCT, 24 had intact superior labra whereas the other six had confirmed SLAP tears at surgery. The sensitivity of the test was 81.8 percent and the specificity was 85.7 percent. The positive predictive value (PPV) was 87.1 percent and the negative predictive value was 80 percent. "Sensitivity" of a test is defined as the probability that patients who truly should have the positive response have that response when the test is performed. When a test has a very high sensitivity, a negative clinical finding effectively rules out the diagnosis. "Specificity" of a test is defined as the probability that patients who should truly have a negative response, express a negative response when the test is performed. PPV is the probability that a patient who receives a positive test result will truly have a positive response (the actual pathology tested for).1 These percentages regarding the PCT are considered very good.
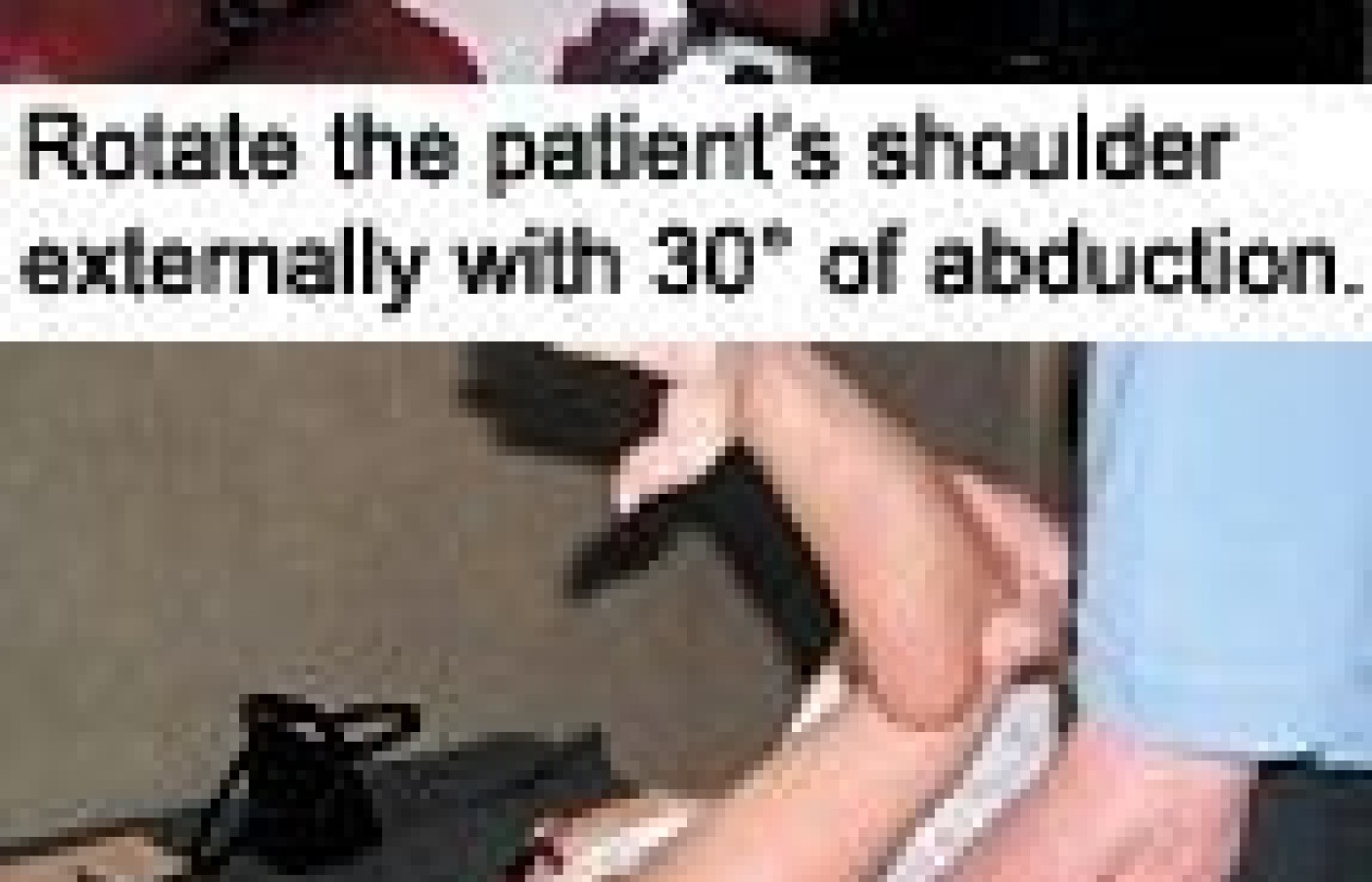
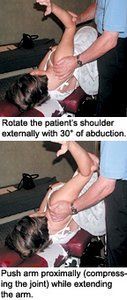
For the PCT, the patient lies sideways on the normal shoulder. The clinician stabilizes the shoulder at the acromioclavicular joint area with one hand and the patient's elbow with the other hand. Next, rotate the patient's shoulder externally with 30 degrees of abduction and then push the arm proximally (compressing the joint) while extending the arm. This should create a passive compression of the superior labrum onto the glenoid. All three motions should be performed at about the same time. The test is positive if it elicits pain or a painful click. The authors feel this test "reenacts the mechanisms of development of SLAP lesions." During external rotation and abduction of the humeral head, the long head of the biceps tendon is pulled laterally and will be under tensile tension as it wraps around the lesser tuberosity. This tension causes the superior labrum to shift from the superior glenoid rim. The second motion of extension of the shoulder with external rotation reproduces the late cocking phase of throwing. These motions have been found to increase the torsional stress at the origin of the long head of the biceps tendon and its attachment to the superior glenoid rim. The compressing of the humeral head "can aggravate the passive displacement of the unstable superior labrum on the glenoid."2 Many SLAP injuries occur due to a fall onto an outstretched arm, creating a compression force to the shoulder.
The authors state that a false-positive result may occur if there is anterior instability of the shoulder determined by the anterior apprehension test or anterior drawer test. So this test will be most accurate if anterior instability is first ruled out. Let us hope that this test remains valid for awhile.
References
Hammer WI. Functional Soft-Tissue Examination and Treatment by Manual Methods, 3rd ed. Sudbury, Mass.: Jones & Bartlett, 2007:33-161.
Yang-Soo Kim, Jung-Man Ha, Kee Yong, et al. The passive compression test: A new clinical test for superior labral tears of the shoulder. Am J Sports Med, 2007;35(9):1489-94.
Guanche CA, Jones DC. Clinical testing for tears of the glenoid labrum. Arthroscopy, 2003;19:517-23.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.