Although plain-film radiographs are commonly acquired by the chiropractor, the abdominal plain film, also known as the abdominal scout or kidney, ureter, bladder (KUB) study, is not typically considered. In actuality, the plain-film abdomen study is very similar to the frontal lumbar spine study routinely performed in chiropractic offices. Although there is a difference in the collimation and the factoring of the lumbar study, essentially all the anatomy visualized on the abdominal plain film can be identified on the abdomen study as well.
Calcifications frequently are found on the lumbar spine study, which can give concern to the practicing chiropractor. The following review of commonly encountered calcifications on plain film is designed to put the practitioner at ease.
To begin, there are two factors that must be considered to assist the interpreter in forming a differential and ultimately a definitive diagnosis. The first factor is the type of calcification; the second factor is the location of the calcification.
Types of Calcifications
Four patterns of calcification can be identified within the abdomen. Each type will present with specific characteristics on X-ray. These calcification patterns assist the interpreter in establishing the differential, and at times, the final diagnosis. The four patterns are concretions, conduit wall calcification, cyst wall calcification and solid mass calcification.1,2,3
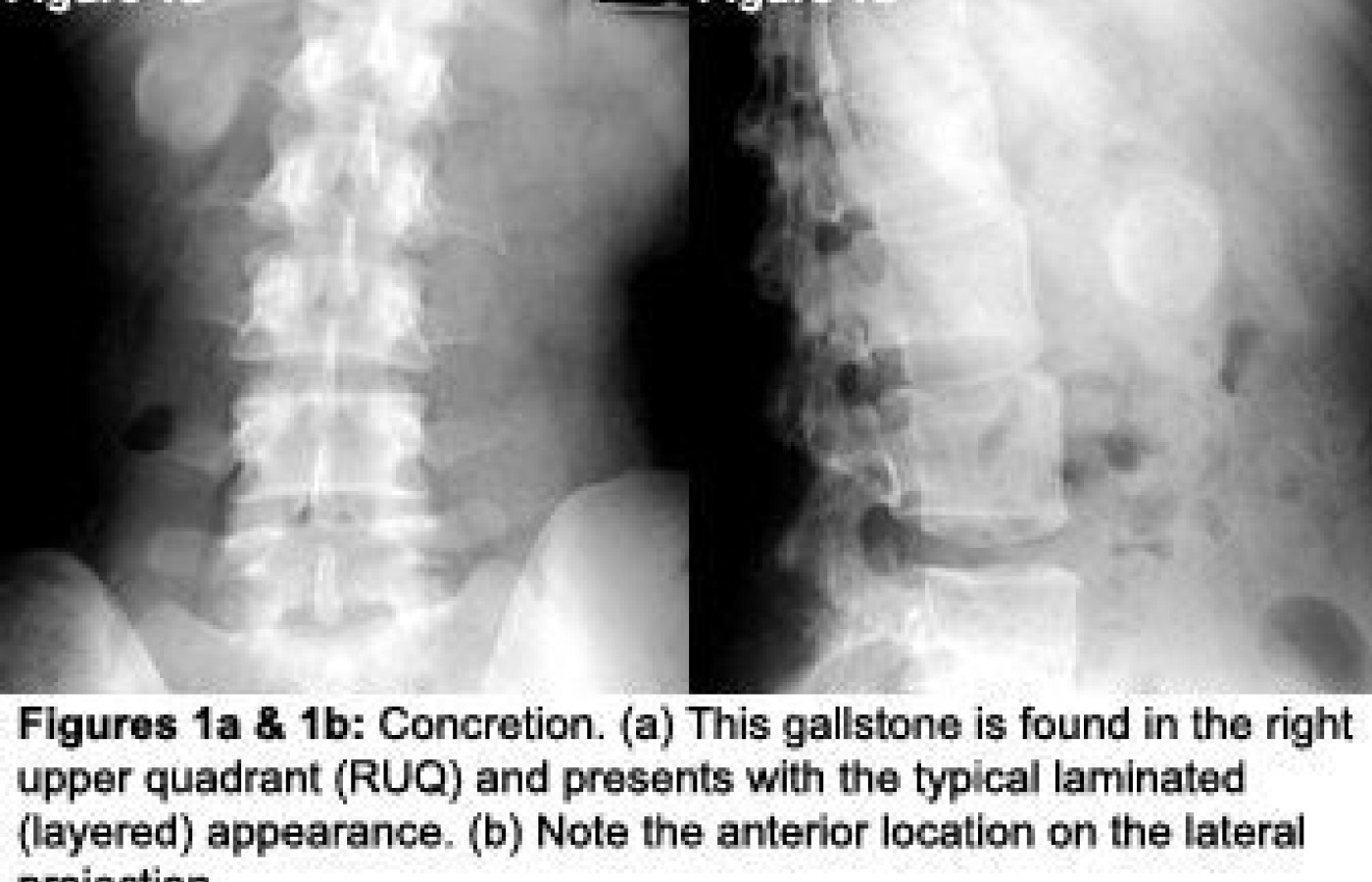
Concretions. These form within a hollow structure. They form because calcium salts fall out of solution, solidify and form a calcified layer on top of a calcified layer. The radiographic pattern of a concretion can vary from a lucent center with minimal calcification, to dense calcification with detailed layers.1,2 They can be either smooth or have irregular borders. Typical structures in which concretions can be found are the gallbladder (gallstones), urinary tract (renal, ureteral or bladder stones), diverticulum/appendix (fecalith, appendicolith), and pelvic veins (phleboliths).1,2,3 The key finding is the layered appearance to the concretion pattern of calcification; once detected, diagnosis is fairly certain (Figures 1a & 1b).
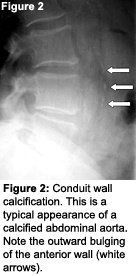
Conduit wall calcification. A conduit is a channel or pipe used for conveying fluids.4 Many conduits are found in the abdomen, including urinary tract, pancreatic ducts, vas deferens, fallopian tubes, biliary ducts and blood vessels.1,2 When the wall of a structure becomes calcified, it presents radiographically as a conduit wall calcification. The pattern and presentation can vary from specks along the route of the wall, to parallel or branching tracks, and even to ring-like densities when seen en face.1,2,3 By far, the most common example of conduit wall calcification is atherosclerotic plaquing of the abdominal aorta (Figure 2).
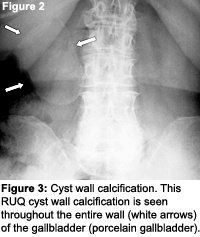
Cyst wall calcification. When the wall of a fluid-filled cyst or hollow organ calcifies, it becomes a cyst wall calcification. An aneurysm of a vessel would actually be included here and not in the conduit wall category. To differentiate between cyst and conduit wall calcification, it is important to establish that the diameter of the calcification is greater than that of the normal conduit. If this is the case, it gets placed in the cyst wall category.1,2 The radiographic pattern of a cyst wall calcification is a curvilinear or arc-like calcification (Figure 3). Structures that may present with cyst wall calcification are aneurysms, the gallbladder and cysts found within solid organs.1,2,3
Solid mass calcification. This fourth and final category can present with a range of radiographic patterns. Often there will be a dense center with irregular margins. They also may present with irregularly shaped, curvilinear, flake-like, streaked or speckled calcific opacities within the mass.1,2 Calcified mesenteric lymph nodes are the most commonly seen mass-type calcifications in the abdomen1,2,3 (Figure 4). Lymph nodes most likely calcify as a result of previous infection, such as tuberculosis. Solid mass calcification also can be seen in the benign uterine fibroma, otherwise known as a leiomyoma (Figures 5a & 5b). These have a "mulberry" pattern of calcification or sometimes a cyst wall-like appearance. Unfortunately, solid mass calcifications can be seen in both benign and malignant processes.1,2,3
Anatomic Location
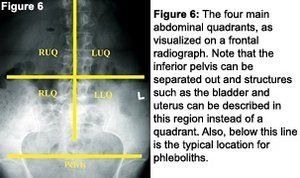
For evaluation purposes, it is best to break the abdomen into four quadrants (Figure 6): right upper quadrant (RUQ), left upper quadrant (LUQ), right lower quadrant (RLQ) and left lower quadrant (LLQ). In addition to the quadrants, the lateral projection will assist in identifying if the object is in the anterior (typically intraperitoneal) or posterior (typically retroperitoneal) location.
The table below5 demonstrates which calcification pattern typically is seen in each respective anatomical structure and where those structures are positioned in the abdomen. A commonly found calcification within the pelvis is the phlebolith. A phlebolith is a stone that forms within the pelvic veins and will present as a concretion in the lower half of the pelvic inlet. It represents an incidental finding and is often not even noted on radiology reports.
Table 1
Quadrant
Peritoneal Location
Anatomic Structure
Calcification Pattern
RUQ
Anterior
Liver
Cyst wall/Mass
RUQ
Anterior
Gallbladder
Concretion
LUQ (most)/RUQ (some)
Posterior (most)
Pancreas
Mass
RUQ/LUQ
Posterior
Adrenal Glands
Cyst wall/Mass
RUQ/LUQ
Posterior
Kidney/Ureter
Cyst wall/Concretion
LUQ
Anterior
Spleen
Cyst wall/Mass
RLQ
Anterior
Appendix
Concretion
RLQ/LLQ/Pelvis
Anterior (most)
Ureter/Bladder
Concretion
RLQ/LLQ/Pelvis
Posterior
Ovary
Cyst wall/Mass
RLQ/LLQ/Pelvis
Posterior (most)
Uterus
Cyst wall/Mass
LUQ/RLQ/LLQ
Anterior
Mesentery
Cyst wall/ Mass
RLQ/LLQ/Pelvis
Anterior
Small Pelvic Vessels
Conduit wall
Conclusion
Categorizing the calcification into one of the four major patterns and locating it anatomically is generally enough to establish a reasonable differential and often a definitive diagnosis. There are times at which there is no clear distinction between patterns of calcification and the presentation doesn't lead in any specific direction. In this scenario, as well as in the course of appropriate follow-up of recognizable calcifications, advanced imaging will most likely be ordered. The best modalities to further assess calcifications within the abdomen are diagnostic ultrasound and computed tomography.1 Both of these modalities will give greater detail in determining the anatomic location and may provide more information with regard to the nature of the calcification.
References
Bassano J. Abdominal calcifications and imaging decision making: a topic review. J Chiro Medicine 2006; 5(1):43-52.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.