I've been using decompression as a spinal treatment during my entire 27-year career. My chiropractic tables, which have served me since I started practice, are two, original McMannis tables - the tables that inspired James Cox to develop his flexion-distraction protocol. I have watched the recent interest in auto-traction, although I will admit to skepticism about a one-size-fits-all solution. Auto-traction has some promising early studies, but may or may not stand the test of time and further research. I've referenced a couple of sites that have reviews of studies of traction at the end of this article.1
First, decompression implies compression, right? Is the lumbar spine compressed? Compression obviously occurs when one sits too long, and can be difficult to recover from with a compromised low back. Another source of compression is excessive long-muscle activity. Think of overactive erector spinae, the hamstrings or the TFL, especially when the smaller core muscles don't know how to work properly in postural activity. Another concept that is useful here is compression versus length. Look at a dancer or anyone with good posture. They hold themselves upright, in length, using the ground and their own musculature to lift upward. They are not resisting gravity; they are utilizing gravity with elegance.
I have had a fascination with long-axis decompression as a direction of adjustment for some time. Most of us tend to focus on rotation, side-bending and flexion-extension, rather than the long axis. I use pressure in the interspinous space, or over the lumbar spinous processes, as indicators of compression, and for the need for a decompression or long axis correction, whether with an adjustment or an exercise. This palpation model is based on limited evidence,2,3 as well as years of experience with the use of this model.
During my years in practice, I have watched various decompression technologies become popular. Flexion-distraction using specially-designed tables (Dr. Cox now calls it Cox Technic) probably started the whole focus on decompression in our profession. Cox Technic has a good Web site and a focus on research, you can see it at [url=http://www.coxtechnic.com]http://www.coxtechnic.com[/url]. Motorized traction tables are another way to apply distraction.
Another tool, not as well-known, is the vertebral distraction pump. What I like about the VDP is its relatively low cost and its ease of use. My article on use of the VDP is at www.chiroweb.com/archives/21/21/09.html. Bruce Broughton, DC, the inventor of this tool, wrote a good article about using this form of distraction on disc herniations.4
I have a personal interest in decompression because I have two torn (internally disrupted) discs, at L4-5 and L5-S1. When I have a flare-up of my discogenic pain, I need decompression.
How often should decompression be applied? In my opinion, as often as needed. When my back is really off, I need decompression as often as twice an hour. On a good day, I should do it at least once daily. So, am I suggesting 365-1,000 adjustments a year? No; I am suggesting you teach your patients how to maintain length and how to decompress themselves with movement and exercise.
When I see these patients in the office, I am going to assess the state of the tissues that contribute to compression - the disc, the posterior ligaments, the erector spinae and the dura mater. I am going to apply some form of adjustment or decompression to each of the involved tissues. The dura has well-thought-out strategies to release it: cranial-type approaches, slow myofascial release aimed at tight places within the dura and its attachments. For the disc, decompression traction of some kind, whether it's an auto-traction device, flexion-distraction table, the vertebral distraction pump and/or just manual pumping. The erector spinae will respond at least temporarily to soft-tissue work. If you don't teach your patients how to activate and utilize their own core, thus inhibiting the erectors, I suspect you may be wasting your time doing soft-tissue work without providing equal attention to retraining the musculature.
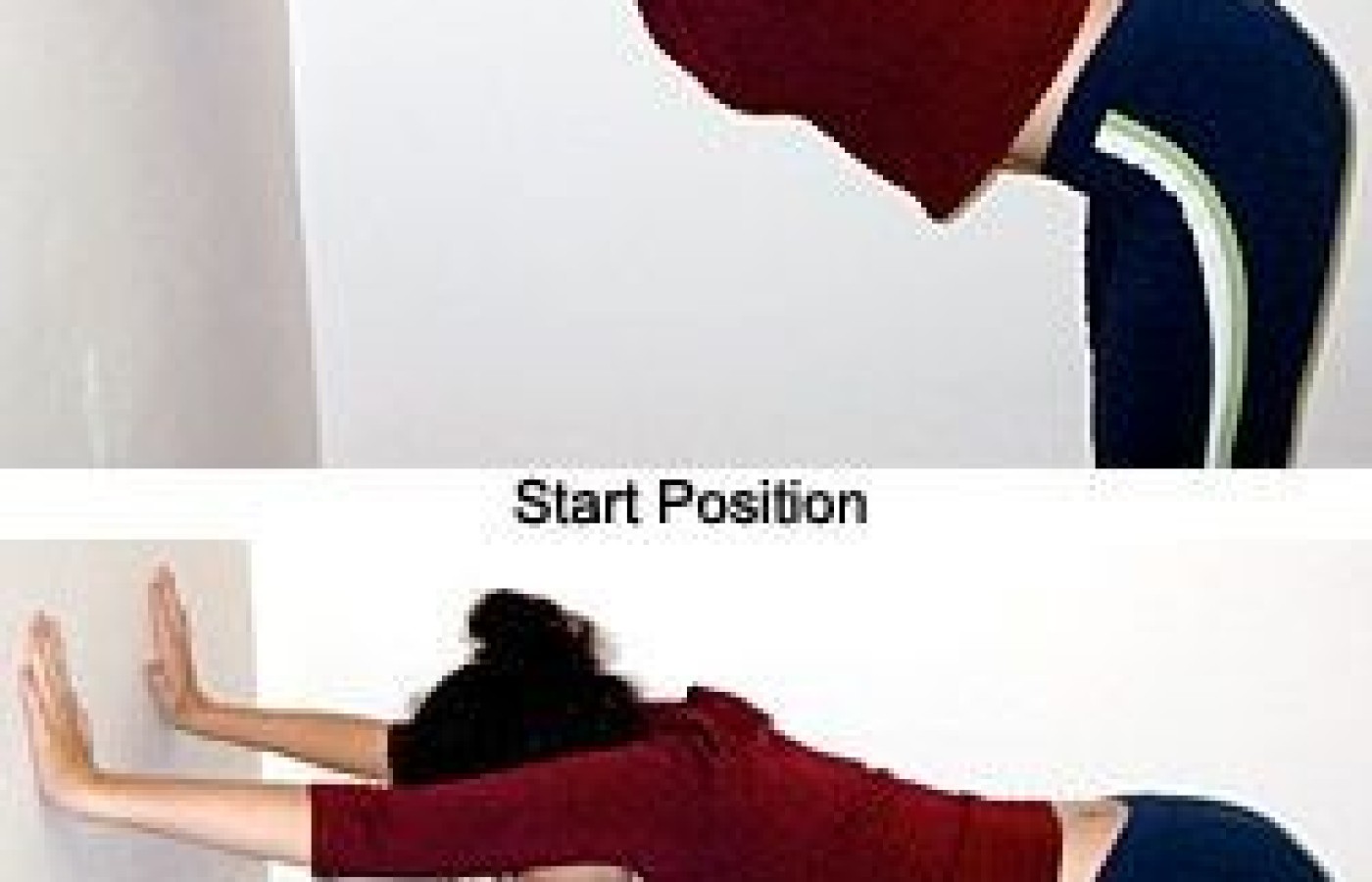
I shared several exercises for low back pain in a previous article.5 One particular exercise, the spine-length squat, is a good decompression exercise. Unfortunately, it's a bit cumbersome and hard to learn, and it requires decent quadriceps strength to use. In this article, I feature another exercise: a modified down-dog (from yoga), pictured at right. I like it because it is easy to use in life, at home and in the work environment. You just need a wall and a desk or counter as aides.
A decompression exercises has several features. It allows the patient to lengthen and stretch their sacrum away from the rest of the spine, while simultaneously demanding they fire their core and maintain lumbar neutral. Sounds like a lot is going on at the same time - yes, there is. You, the doctor/teacher, have to be motivated. The patient has to be motivated, which your enthusiasm can help. Patients in pain also have to get through the fear that can block them from moving forward, both figuratively and literally.
I'll outline the steps to get into the modified down-dog, wall version. Stand with the hands shoulder-width apart. Pull your elbows isometrically in toward your head. Drop your shoulder blades and chest toward the floor. Keep your knees bent enough to allow you to stay in lumbar neutral. The head stays neutral, not looking up or hanging down. Pull in with your lower belly. Actively push your bottom away from the wall. (For some, pushing away from the wall gets the traction activated, for others a better cue is to tell them to tuck the tailbone, while maintaining neutral. The "tuck" is almost isometric; the body positioning and core activation prevents lumbar flexion.) Hold the position for 20-60 seconds while breathing, and then repeat two or three times. Bend the knees further as you begin to come up, for safety. This exercise, when done correctly, is safe and useful for beginners or less motivated patients. Patients who understand their core will get even more out of this positioning.
The second exercise pictured, modified down-dog, counter version, is quite similar, except that you are using a countertop to rest your hands on. This may be a little scary at first, as you are lower and more bent forward; keep the knees bent to keep the spine in neutral. Another variation on this one is to grab the back of the countertop or railing, giving you something to pull against to emphasize the traction. I've placed a pdf of this exercise, for use as a handout, on my Web page; see www.marchellerdc.com/rehab_exercise.htm.
I have found an excellent way to motivate the patient to use this exercise. When I find a patient with midline tenderness in the lower lumbar spine, I have them get up off the table and come over to the wall. I'll have them do this exercise for 20 seconds, coaching them to do it right. They then lie down again and I repalpate for the midline tenderness. It's almost always somewhat better, often dramatically so. The patient now knows they can help themselves when they get compressed. You can use the same principle to test another exercise, such as Mackenzie extension, for its immediate effect on the compression pattern.
References
www.cochrane.org/reviews/en/ab003010.html and www.lni.wa.govclaimsins/files/omd/vaxdta.pdf.
Yrjama M, Tervonen O, Kurunlahti M, Vanharanta H. Bony vibration stimulation test combined with magnetic resonance imaging. Can discography be replaced? Spine 1997;22(7):808-13.
Vanharanta H, Ohnmeiss D, Aprill C. Vibration pain provocation can improve the specificity of MRI in the diagnosis of symptomatic lumbar disc rupture. Clin J Pain 1998;14:239-247.
Broughton, Bruce, Treatment of disc herniations with the distraction pump. Chiropractic Technique, May 1999;11(2).
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.