Treatment of the Distal Fibular for Lateral Ankle Sprains
Warren Hammer, MS, DC, DABCO
Mulligan1 believes the most significant lesion in a lateral ankle inversion sprain is due to the distal fibula getting "wrenched forward on the tibia," creating a positional fault. He feels that the lateral ligamentous damage is "usually insignificantly damaged." A recent article in the Journal of Orthopaedic & Sports Physical Therapy confirms his findings.2 The authors of the study compared 30 patients who had no history of ankle sprain with 30 patients who had chronic ankle instability (CAI). The authors concluded that "the fibula was positioned significantly more anterior in relation to the tibia in subjects with unilateral CAI. It is unclear if repetitive bouts of ankle instability
caused the anterior fibular position or if the more anterior position was a predisposing factor to injury." Mavi, et al., used MRI to measure and also found the fibula positioned more anteriorly in an injured group.3 Other studies have found the fibula to be posterior positioned in acute ankle sprains; but Hubbard, et al.,argue that the other measurements compared the fibular position to the talus rather than to the tibia.2
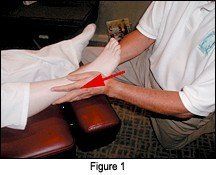
I recently used the Mulligan procedure for an acute lateral ankle sprain with excellent results. The patient had a typical inversion plantar flexion sprain with moderate swelling on the lateral side. Mulligan recommends immediate repositioning of the fibulal.1 You can first test the area to see if repositioning will help. With your left thenar eminence on the patient's right foot, put your other hand around the Achilles' tendon to stabilize the distal leg, and then use a posterior/superior force on the distal lateral malleolus (Figure 1)
Hold this contact and notice if active inversion by the patient is relieved. If there is not marked relief, change the angle of your glide to reach the least painful motion during the active patient inversion. Taping is next, and after 48 hours, this test motion can be used with Mulligan's "mobilization with movement" method, in which the practitioner glides the lateral malleolus posterior/superior while the patient actively moves the foot into inversion/plantar flexion without pain. At the end of the inversion/plantar flexion, the patient or practitioner can contact the foot and use overpressure in inversion while the practitioner holds the contact.
Apply 2-inch-wide tape while the foot is in a neutral position anterior to the distal fibula with the tip of the distal fibula exposed below the tape's edge (Figure 2). Tape in the posterior/superior direction and maintain the posterior/superior pressure while the tape is pulled around the distal leg. Make sure the tapes do not meet, as space may be needed for possible swelling. While not shown, it is a good idea to reinforce the taping with a second strip. The tape may be changed every 48 hours.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.