In one of last year's columns, I dealt with the problems surrounding the use of progress notes in a busy chiropractic practice and discussed the concept of the daily patient record. The daily patient record provided the patient several methods for documenting the level of pain currently being experienced through the use of the visual analog scale and the "dollar's worth of pain" analogy. Furthermore, through the use of the pain drawing, the daily patient record provided a means of obtaining a visual record for the patient's current pain.
The current discussion will center around a more detailed examination of the use of the pain drawing. Pain drawings provide the physician with a means of quickly assessing the patient's levels of pain. The pain drawing can demonstrate whether the patient is demonstrating symptoms consistent with an organic lesion, whether the patient is amplifying pain levels, or if there are non-organic factors involved in the patient's case. Several pain drawings rating systems have been proposed for the analysis of pain drawings.
The following rating system was proposed by Hildebrandt1 and provides the physician with a means of numerically rating the pain drawing. This system was a modified version of the system originally proposed by Ransford.2
Scoring System for Pain Drawings
I. Unreal drawings. If one or more of the following pain localizations are drawn in, two points are assigned.
A. Total leg pain B. Frontal aspect of one or both legs C. Unilateral or bilateral anterior tibial pain D. Back of leg (isolated, knee included) E. Circumferential thigh pain
F. Lateral whole leg pain (trochanteric area and lateral thigh allowed) G. Bilateral foot pain H. Circumferential foot pain I. Anterior knee pain, ankle pain J. Spotted bounds of pain scattered about the whole leg K. Whole abdomen pain
II. Drawings showing "expansion" or "magnification" of pain (one or two points per area, depending upon extent)
A. Back pain radiating to the iliac crest, groin, or anterior perineum (coccygeal pain allowed). Note: Rule out sacroiliac joint dysfunction.
B. Pain drawn outside the outline as an indication of magnification.
III. "I particularly hurt here" indicators (each category scores one point.
A. Additional explanatory notes B. Circle painful areas C. Draw lines to demarcate painful areas
D. Use arrows to describe anatomically not explainable pain E. Use of additional symbols
IV. "Look how bad I am" indicators. (Score one with small areas and score two with larger areas.)
A. Additional painful areas in the trunk, head, neck, or upper extremity dawn in.
With this rating system, a score of three or more is generally thought to represent a pain perception that may be influenced by psychological factors. Some of the readily apparent expressions of psychological distress include pain distributions that are non-anatomic or bizarre, drawings showing "magnification" or "expansion" of symptoms, and drawings that demonstrate "look how bad I am indicators."
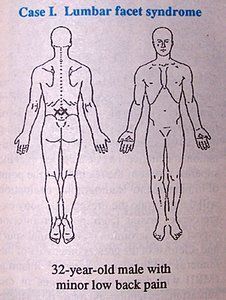
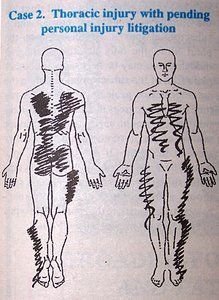
Uden3 proposed an observational system for assessment of pain drawings. Uden's system relies on the impression formed by physicians familiar with low back disorders, who categorize the drawings into one of four categories: organic, possibly organic, possibly non-organic, or non-organic. This rating system demonstrated that even when one is inexperienced with the use of pain drawings, the intraexaminer reliability was 80 percent and the interexaminer reliability was 70 percent. By using one of these two systems for rating the pain drawing, the clinician can gain insight into the possibility of the presence of psychological distress which may complicate the patient's case. The following cases are provided as examples of pain drawings for various cases:
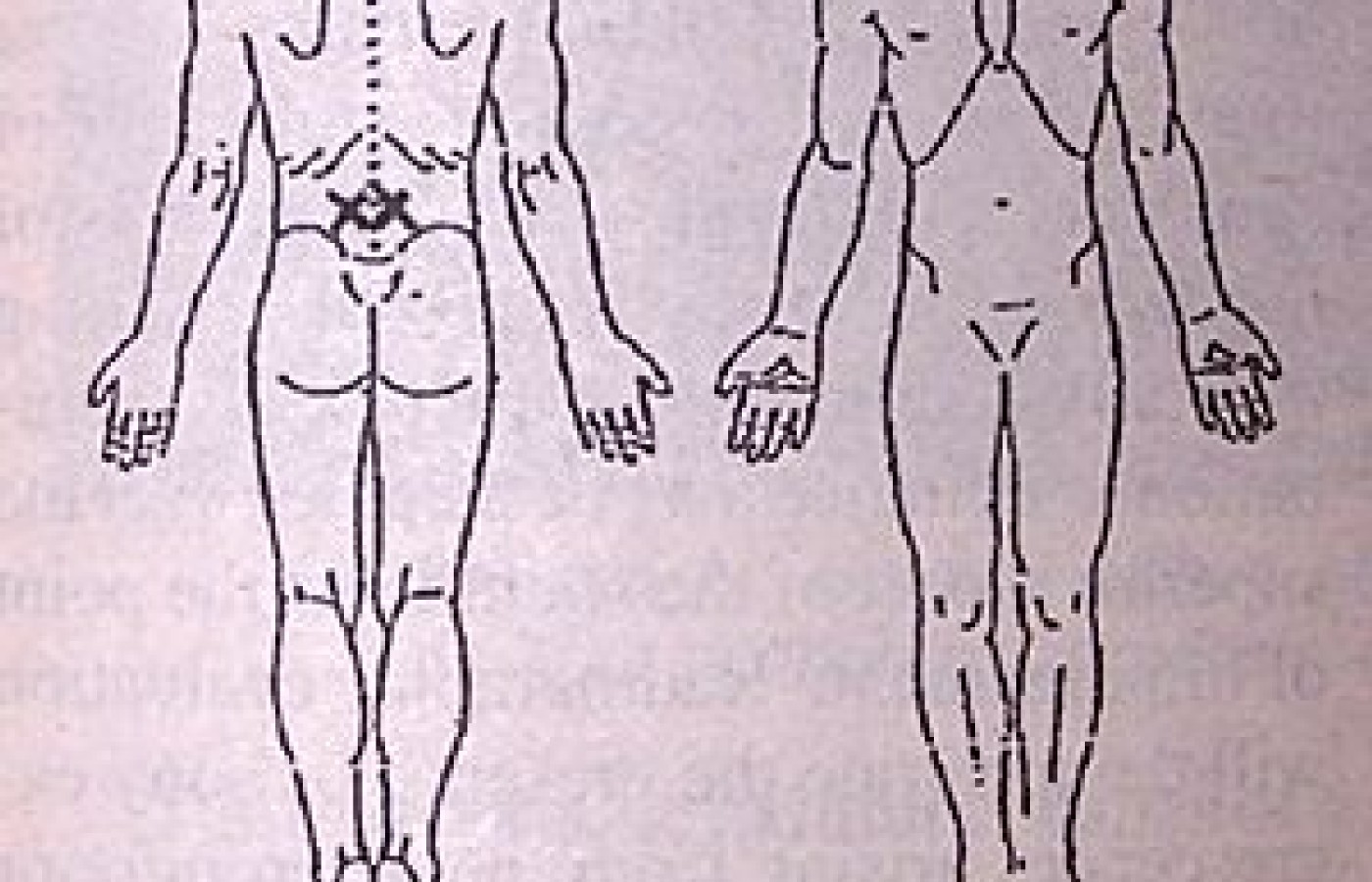
34-year-old female who was injured in a grocery store parking lot. Through cursory observation, this pain drawing has a "non-organic" appearance. Through the pain drawing scoring system, this drawing received a score of 8.
2 points for frontal aspect of one or both legs
2 points for pain outside the lines
2 points for pain radiating into the iliac crest (no sacroiliac dysfunction noted on exam)
2 points for additional painful areas drawn in
References
Hildebrandt J, et al: The use of pain drawings in screening for psychological involvement in complaints of low back pain. Spine, 13(6):1988.
Ransford AO, Cairns D, Mooney V: The pain drawing as an aid to the psychological evaluation of patients with low back pain. Spine, 1(1):1976.
Uden A, et al: Pain drawings in chronic back pain. Spine, 13(4): 1988.
Goldman, Sherwin, and Merritt JL: Using pain drawing in evaluating low back disorder. Journal of Musculoskeletal Medicine, August 1991.
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.