The RPSP is a pattern of muscle dominance resulting from the habitual, repetitive use of the same muscles every time we engage in any posture. It is rare that we will use the same muscles on both sides of our body in the same manner. Thus, we create a pattern of muscle use on each side that is different than the pattern of use on the other side (Figure 1). We refer to the overall pattern of habitual, repetitive use as the RPSP. We call the overall pattern of infrequent use the contra pattern (mirror image of RPSP).
Figure 1 One of 32 known Repetitive Posture Stress Patterns (posterior view).
Which Postures Create the RPSP?
All postures contribute to the RPSP. The four postures all people engage in are the primary postures of reclining (sleeping), sitting, standing, and walking. We sleep with one arm and one leg positioned differently than the others. We prefer to cross one leg more than the other when we sit. We stand on one leg differently than we stand on the other. We walk on one leg differently than we walk on the other. During work and play we unconsciously use those muscles made dominant from habitual use in the primary postures.
Our postural idiosyncrasies begin to develop in utero. During this time we develop a preference for positioning one arm and leg differently than the others. By the time we reach the age of 12 to 18 months, we have developed our own specific primary postures, i.e., dominant limbs, which continue, with certain modifications for growth, virtually unchanged throughout life.
Since the RPSP Is Caused by Normal Activities, Why the Concern?
Whenever muscles are activated in dynamic use, static positioning, or therapeutic release, the entire skeletal system moves in response to the change in length of the muscle fibers, i.e., any action, such as the active lifting of a leg or the passive stroke of a muscle, as in reflex testing, produces changed in the entire kinematic chain. If the activated muscles increase the strength differential from one side to the other, as in the use of the RPSP, the skeletal system moves away from balance. If the activated muscles decrease the strength differential from one side to the other, as in the use of the contra pattern, the skeletal system moves toward balance. The direction of movement can be observed by monitoring various skeletal checkpoints before and after activation.
There would be no cause for concern if the RPSP was used only slightly more than the contra pattern. However, the RPSP is used in most instances because it is comfortable to use and the contra pattern is not. For example, a person will cross one leg (RPSP) comfortably when sitting, but the other leg will feel tighter and less comfortable when it is crossed. Therefore, the uncomfortable leg (contra pattern) will be crossed much less often. Similar tendencies can also be found in sleeping, standing, walking, working, and playing. Day after day, the skeletal system is being postured deeper and deeper into misalignment patterns, and will eventually have a negative effect, particularly on the nervous system.
The depth of the misalignment is usually not apparent when using one of our most common analytical tests -- leg length inequality. This is because unbalanced postural activities both shorten and lengthen each leg. The net result may manifest as one-quarter inch leg length inequality because the apparent long leg happened to lengthen one inch and shorten three-quarters of an inch during unbalanced postural activity, while the apparent short leg lengthened and shortened half inch in each direction. The net effect would be a quarter inch short leg and varying degrees of misalignment throughout the skeletal system. The apparent short leg frequently becomes the apparent long leg during the RPSP release procedure, before returning to an equal length. It is my experience that more trigger points and areas of myofascitis are found in the RPSP than in the contra pattern, contributing to the depth of the skeletal misalignment pattern.
The most important unbalanced structures are the extremities, because of the time spent in unbalanced use and their relative power. An example of the influence unbalanced extremities can have on the spine is illustrated by the consistent alleviation of certain types of torticolis seen following the release of the RPSP, without adjusting the cervical spine. They can also be made worse by releasing the contra pattern of the extremities. Just as the RPSP is little understood and universally common, so are pain syndromes and many other health problems.
What Can Be Done to Stop Using the RPSP and Begin Using the Contra Pattern?
I have been investigating the RPSP for 12 years, and have devised an analytical method to determine an individual's specific RPSP. Once the RPSP is known, the data can be used for three distinct approaches, all contributing to the same goal -- movement of the skeletal system toward alignment along the same path it traveled in its migration toward misalignment, and correction of the vertebral subluxations:
release of the RPSP
adjusting in opposition to the RPSP
strengthening of the contra pattern
Many chiropractors view absolute skeletal balance as unattainable. I share the same view. Note that the use of the word balance is always preceded by "toward" and/or "away from" to indicate direction of movement only. Muscle use, soft tissue therapy, or osseous adjustments will cause movement of the entire skeletal system either away from or toward balance. The objective, when working with the RPSP, is always to avoid the former and promote the latter.
Release of the RPSP consists of applying a muscle releasing modality to the individual's specific pattern. Release of the shortened muscle fibers allows the skeletal system to move toward balance, equalizing bilateral skeletal checkpoints (leg deficiency, crests of the ilia, inferior scapular angles, arm deficiency, and mastoid processes). At the same time, many subluxations are automatically reduced, improving the nerve deficit, and relieving many symptoms.
The direction of spinal misalignment is generally, but not specifically, the same in individuals that have the same RPSP. Variations can be attributed to the degree of the particular individual's posture imbalances, as well as the genetically determined quantity and quality of muscle distribution peculiar to that particular race, nationality, or individual. However, certain known directional tendencies, plus reflex testing, makes it possible to adjust the spinal column using a line of correction that reinforces the skeletal position achieved by the release of the RPSP.
To maintain the new skeletal position, the patient must stop using the RPSP and begin using, and strengthening, the contra pattern. This is done by reverse posturing which must be taught to the patient. The effects of reverse posturing are manifested by the continued elimination of apparent leg and arm deficiency, and continued maintenance of level crests of ilia, inferior scapular angles, and mastoid processes.
The most popular prescription for musculoskeletal rehabilitation is exercise. However, exercise has positive and negative effects on the musculoskeletal system. The positive effect can be increased muscle strength or endurance. The negative can be increased skeletal misalignment due to our habit of using the RPSP more than the contra pattern. Completing each exercise routine with unilateral exercises of the contra pattern will minimize skeletal misalignment.
How Does this Hypothesis Contrast to Current Chiropractic Thinking?
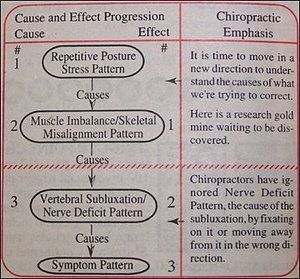
The dichotomy within the chiropractic profession has one group focusing on the vertebral subluxation and totally excluding soft tissue work in their effort to correct it. The other group includes soft tissue work using the allopathic model, i.e., treatment of the symptomatic area. These preoccupations have prevented us from making even a minimal effort to understand the cause of what we are trying to correct (Figure 2). Neither group has directed its thinking toward the dynamic aspects of the myofascialskeletal system as a functional unit in its function of relating the organism to gravity.
Figure 2
The RPSP hypothesis indicates that you cannot separate the myofascialskeletal system anatomically or functionally. When myofascia is contracted or released, by use or therapy, the entire skeletal system moves toward or away from balance. The same phenomenon results from adjusting any major articulation, including those of the spinal column. Following is an important premise that is a constant when working with the myofascial system: The direction of movement of the skeletal system seen when a muscle is activated (contracted or released) will be the opposite of that seen when the same contralateral muscle is activated in the same way. The direction of movement of the skeletal system seen when a muscle is activated will be the same as that seen when the same contralateral muscle is activated in the opposite way. Movement of the skeletal system may not be detected following activation of muscle if the same contralateral muscle as that being activated is of equal strength.
Assume any posture using muscles that are stronger than their contralateral partners and the entire skeletal system will move away from balance. Assume any posture using muscles that are weaker than their contralateral partners and the entire skeletal system will move toward balance.
Apply soft tissue releasing therapy (ultrasound, electrotherapy, massage, trigger point therapy, acupressure, etc.) to muscles that are stronger (RPSP) than their contralateral partners and the entire skeletal system will move toward balance. Apply soft tissue therapy to muscles that are weaker (contra pattern) than their contralateral partners and the entire skeletal system will move away from balance.
Adjust any articulation in the proper direction and the entire skeletal system will move toward balance. Adjust any articulation in the wrong direction and the entire skeletal system will move away from balance.
Movement toward balance corrects subluxations and/or impedes their development. Movement away from balance creates subluxations and/or furthers their development. This innovative approach, used exclusively by RPSP to correct subluxations and maximize movement of the skeletal system toward balance, yields fast and consistent structural and symptomatic changes and teaches the patient a unique way to minimize recurrences.
Muscle use, soft tissue therapy, and osseous adjustments are the methods of choice commonly used by the various disciplines for musculoskeletal conditions. Could it be that all disciplines are intentionally or unintentionally removing and/or creating nerve interference by modifying the relationship of the skeletal system to the nerve system and, in doing so, removing and/or creating subluxations?
Raffael Siclare, DC 1719 Woodbine Place Oceanside, CA 92054 Phone: (619) 722-2525 Fax: (619) 722-2273
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.