About the authors: Dr. Keld Ostergaard, a 1990 graduate of the Anglo-European Chiropractic College, has been in private practice since 1991. He received his MD from the University of Copenhagen (1995), and that institution's gold medal for research (1994) in molecular biology and osteoarthritis. He is co-editor of the journal of the Danish Chiropractic Assoc., and an FCER research fellow. His articles on rehabilitation and assessment of the low back and neck have been published in the Journal of Musculoskeletal Pain, in the journal, Pain, and in Spine (June, 1995 editorial). The Jan. 1996 issue of JMPT featured his double article on neck/shoulder rehabilitation. Dr. Ostergaard is pursuing his doctorate at the University of Copenhagen.
Dr. Alan Jordan is a 1979 graduate of the Canadian Memorial Chiropractic College, and has been in private practice since that time. He is in his final year of a doctoral program at the University of Copenhagen's National University Hospital. He is a research fellow of the FCER and the Danish Chiropractic Assoc., and has been a consultant to Denmark's Dept. of Health.
In our first article regarding the topic of rehabilitation in chiropractic clinics (Jan. 1, 1995, "DC"), we reviewed what we felt were the most compelling reasons for chiropractors to incorporate rehabilitation in their overall treatment strategies for patients suffering both chronic and recurrent spinal pain. We presented some of the international developments in rehabilitation and emphasized that excellent clinical results could be obtained without employing high-tech and prohibitably expensive equipment. In this article we will discuss the essential aspects of program design for low back rehabilitative protocols.
Trends in Low Back Rehabilitation
Patients suffering from low back pain have received advice regarding exercise programs from health care workers for hundreds of years. The design of these programs has been largely based upon empirical considerations, and only in the recent past have researchers begun to scrutinize the validity of exercise for low back pain and program design.1 Research studies have clearly demonstrated that the clinical results obtained from exercise programs undertaken in clinics and under constant supervision are clearly superior to those programs carried out outside of the clinical setting.2 Patient compliance is extremely poor when subjects are not monitored. Effective training requires equipment so that the elementary principles of rehabilitation including progressive resistance can be adhered to while patient safety is maintained. Patients who have suffered low back pain for longer periods of time need encouragement and guidance from instructors and they feel secure training at the clinics where knowledge of their particular case is greatest.
During the '70s and early '80s, there was a theoretical debate going on between adherents of William's protocol, which emphasized strengthening of the abdominal musculature and stretching of the posterior musculature, and proponents of McKenzie's protocol, which emphasized training the posterior musculature of the spine. It is beyond the scope of this paper to review the debate, but as with so much else in physical medicine it needed to be put to the test. Two studies involving both acute and chronic patients clearly demonstrated that strengthening the extensors of the spine as opposed to the abdominal musculature resulted in superior results.3,4 Since that time the clinical studies of Claus Manniche MD, PhD and others, have clearly demonstrated that excellent results can be obtained on both chronic and postoperative patients by strengthening primarily the posterior musculature.1
A recent study has shown that manipulation combined with extension exercises resulted in superior results to those obtained through exercise alone.5 Functional assessment of patient populations compared with matched healthy individuals repeatedly points to decreased strength levels of the posterior musculature, resulting in patients which are "flexor powered."6 In the healthy population the extension to flexion strength ratio is approximately 1.5 to 1. Patient populations demonstrate one to one extension to flexion ratios, thus indicating that the greatest strength losses occur in the posterior musculature.6 Epidemiological studies have also shown that reduced endurance levels of the extensors predispose patients to repeated episodes of low back pain,7 as well as healthy individuals involved in heavy work tasks who have not experienced previous low back pain.8
Although research authorities recommend strengthening both the extensors and the abdominal musculature,1 clearly the emphasis must be placed on strengthening the extensor musculature.
Another aspect of exercise that has resulted in debate among health professionals is the type of exercise patients should be doing. Here the debate has revolved around whether patients should be doing their exercises isometrically, isotonically, isokinetically, and so forth. After Nachemsom and Elfstrom published their disc pressure measurements in the early '70s,9 health workers reverted to isometric exercise to decrease the possible increases in discal pressure which could result from dynamic exercise. A few studies published in the '60s resulted in positive results,10,11 but clearly the trend today is towards full range of motion dynamic exercise.1 This provides increased blood perfusion to the muscles and increases strength throughout the range of motion trained. Additionally, the many published studies utilizing dynamic exercise report exceedingly few negative side-effects from dynamic exercise. At the present time there is no evidence that superior results can be obtained through predetermined speeds during training, such as those employed in isokinetic training.
Designing a Low Back Exercise Program
Exercise programs can be divided into three major phases.
The first is the warm up phase, requiring 10-15 minutes. Here patients increase body temperature by stationary bicycling or on step machines. This should be carried out for 6-8 minutes. Increased body temperature increases tissue elasticity and blood is channeled to the musculature. Afterwards all relevant muscles should be stretched in preparation for strength training.
The second phase involves strengthening of the muscles which the chiropractor has determined necessary. In this article we will concentrate on the extensors of the spine, as we feel that they are the most important muscle group requiring rehabilitation. This period usually lasts 35-45 minutes. The extensors can be strengthened in both the sitting position or in the prone position. Exercising the extensors of the spine in the sitting position is usually carried out in specially designed training machines with resistance and isolation of the extensor muscles. The resistance may be variable and patients are generally seated in fixed positions.
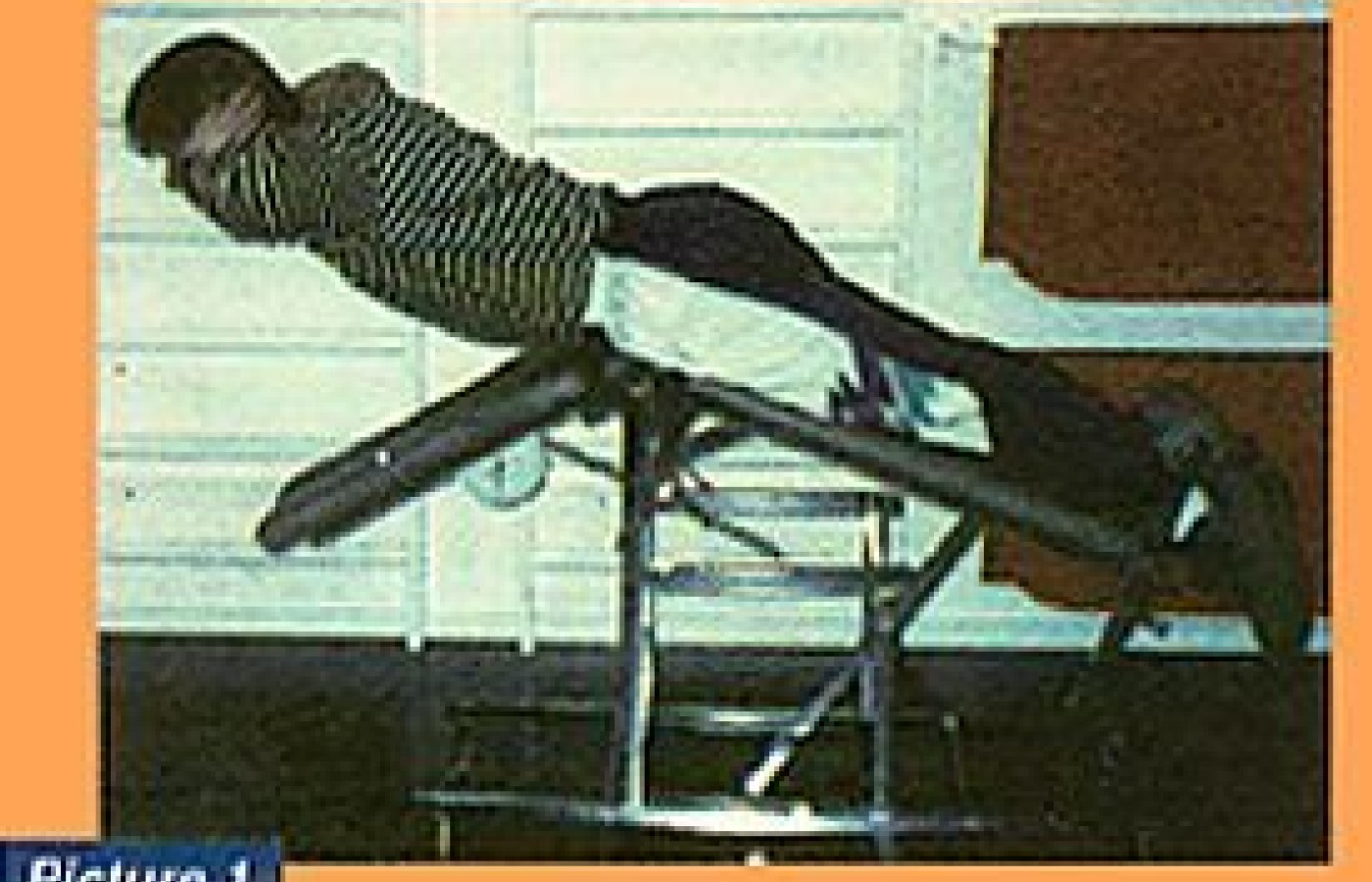
Another way to strengthen the extensors is in the prone position (Picture 1). This has the advantage of improving the coordination of the different muscle groups involved in lifting. The first muscles to be activated are the hamstrings, followed by the gluteals, and finally the extensors of the spine. On the way down the opposite sequence takes place. This motion duplicates placing an object on the floor and thus provides another valuable coordination improvement. For most patients the resistance level with this type of exercise is roughly 30-35 percent of their maximal capabilities. This is the ideal level for endurance training and provides for maximal blood perfusion and healing. Progressive resistance can be provided by asking the patients to carry weights in their arms or by providing them with vests which contain weights. Patients begin at approximately 30 to 40 repetitions in series of 10, resting for 1-2 minutes between series, and gradually increasing to approximately 100 repetitions during a three month period.
Patients who have difficulty carrying out an extension can be assisted by an instructor until they can manage themselves. This type of training is ideal to overcome fear avoidance, but should not be continued for more that a few weeks.
Hyperextension (Picture 2) has been the subject of heated debate. After having trained hundreds of subjects and having conferred with others in rehabilitation we feel that there is not much to be gained by hyperextending much more that 20-25 degrees over the horizontal. One need not be hysterical however about extending over the horizontal because to strengthen the segmental musculature some extension over zero degrees is necessary. In a future article regarding the effect of training on different tissue types we will expand on hyperextension and its particular effect on the discs of the spine.
Other muscles requiring training include the gluteals, the quadriceps and the abdominals. Fitness training may be integrated but is not a necessity.
The concluding phase of each training session should include relaxation and stretching of the trained muscles. This cool-down phase should last for approximately 10 minutes making the entire session somewhere between one hour and 15 minutes to one hour and 30 minutes.
Most chronic patients will require 2-3 training sessions per week for a period of at least three months. Some patients will require more time depending upon the duration and severity of symptoms and progress during rehabilitative procedures. It is not unusual for rehabilitation to require upwards of six months to maximize both objective and subjective gains.
The majority of chronic low back patients, or those suffering recurring pain, require rehabilitation. The most logical place for rehabilitation is in the clinical setting.
In future articles we will discuss among other topics contraindications and possible side-effects to rehabilitation, patient selection and expectations, monitoring results and other relevant aspects of rehabilitation in the chiropractic clinical setting.
References
Manniche C. Assessment and exercise in low back pain. Doctoral thesis. Laeforenings Forlag. Copenhagen 1995.
Reilly K, Lovejoy B, Williams R, Roth H. Differences between a supervised and independent strength and conditioning program with chronic low back syndromes. J Occup Med 1989; 31: 547-50.
Nwuga G, Nwuga V. Relative therapeutic efficacy of the Williams and McKenzie protocols in back pain management. Physio Prac 1985; 99-103.
Donelson R, Grant W, Kamps C, Medcalf R. Pain response to sagittal end range spinal motion: A prospective, randomized, multicentered trial. Spine 1991; 16: 206-12.
Erhard RE, Delitto A, Cibulka M. Relative effectiveness of an extension program and a combined program of manipulation and flexion and extension exercises in patients with acute low back syndrome. Physical Therapy 1994; 74: 1093-99.
Beimborn DS. Morrisey MC. A review of the literature related to trunk performance. Spine 1988; 13: 655-60.
Biering-Sorensen F. Physical measurements as risk indicators for low-back trouble over a one-year period. Spine 1984; 9: 106-19.
Luoto S, Heliovaara M, Hurri H, Alantra H. Static endurance and the risk of low-back pain. Clinical Biomechanics 1995; 10: 323-324.
Nachemson A, Elfstrom G. Intravital dynamic pressure measurement in lumbar discs. Scandinavian J of Rehab Med. 1970; suppl 1: 1-40.
Kendall Ph, Jenkins JM. Exercises for backache: A double-blind controlled trial. Physiotherapy 1968; 54: 154-7.
Lindstrom A, Zachrisson M. Physical therapy on low back pain and sciatica. Scand J Rehab Med 1970; 2: 37-42.
Alan Jordan, DC Keld Ostergaard, DC, MD Farum, Denmark
The chiropractic profession is under a sophisticated and relentless assault from corporate medicine, so strategically executed that most don’t even recognize it happening. The campaign is powerful, calculated, and well-funded, demonstrated by its covert tactics and the millions being invested to carry it out. Corporate medicine's endgame wants only two things from chiropractic: all our patients and all our money – and it is getting it.
Over the past two decades, more than 18 million spinal surgeries have been performed in the United States, and cervical disc replacements represent a fair share of those. Device recalls due to design flaws can place patients in difficult clinical situations, especially those who are symptomatic and reluctant to undergo revision surgery. This case highlights the role of chiropractors in managing complex postsurgical patients, particularly those with recalled spinal implants.
UnitedHealth Group, parent company of UnitedHealthcare, has announced sweeping changes to its prior-authorization (PA) requirements that will eliminate the requirement for chiropractic care and numerous other healthcare services by the end of 2026. Doctors of chiropractic, other providers and patients have long lamented prior authorization requirements because they can delay needed treatment, limit access and even cause some patients not to pursue care.