The Chasm Between Posture and Chiropractic Education and Treatment
David Seaman, DC, MS, DABCN;
Steve Troyanovich, DC
Abnormalities of posture are common cause of pain and disability often overlooked by practitioners who treat patients suffering from acute and chronic musculoskeletal complaints.1-5 Kendall states: "Postural faults that persist can give rise to discomfort, pain, or disability. The range of effect from discomfort to incapacitating disability is related to the severity and persistence of the faults."6
Believe it or not, in 1947, the American Academy of Orthopaedic Surgeons (AAOS) had a posture committee. According to Kendall, the AAOS definition of poor posture is ". . . a faulty relationship of the various parts of the body which produces increased strain on the supporting structures and in which there is less efficient balance of the body over its base of support."6
Addressing poor posture is an important issue, and it is typically neglected in chiropractic education and clinical practice. Do you remember the class you had in chiropractic college that was exclusively devoted to assessing and restoring normal posture? We don't.
Despite this lack of formal education, most DCs still acknowledge the importance of good posture, as did the AAOS in 1949 with this definition: "Good posture is that state of muscular and skeletal balance which protects the supporting structures of the body against injury or progressive deformity irrespective of the attitude (erect, lying, squatting, stooping) in which these structures are working or resting. Under such conditions the muscles will function most efficiently and the optimum positions are afforded for the thoracic and abdominal organs."
What Constitutes Good Posture?
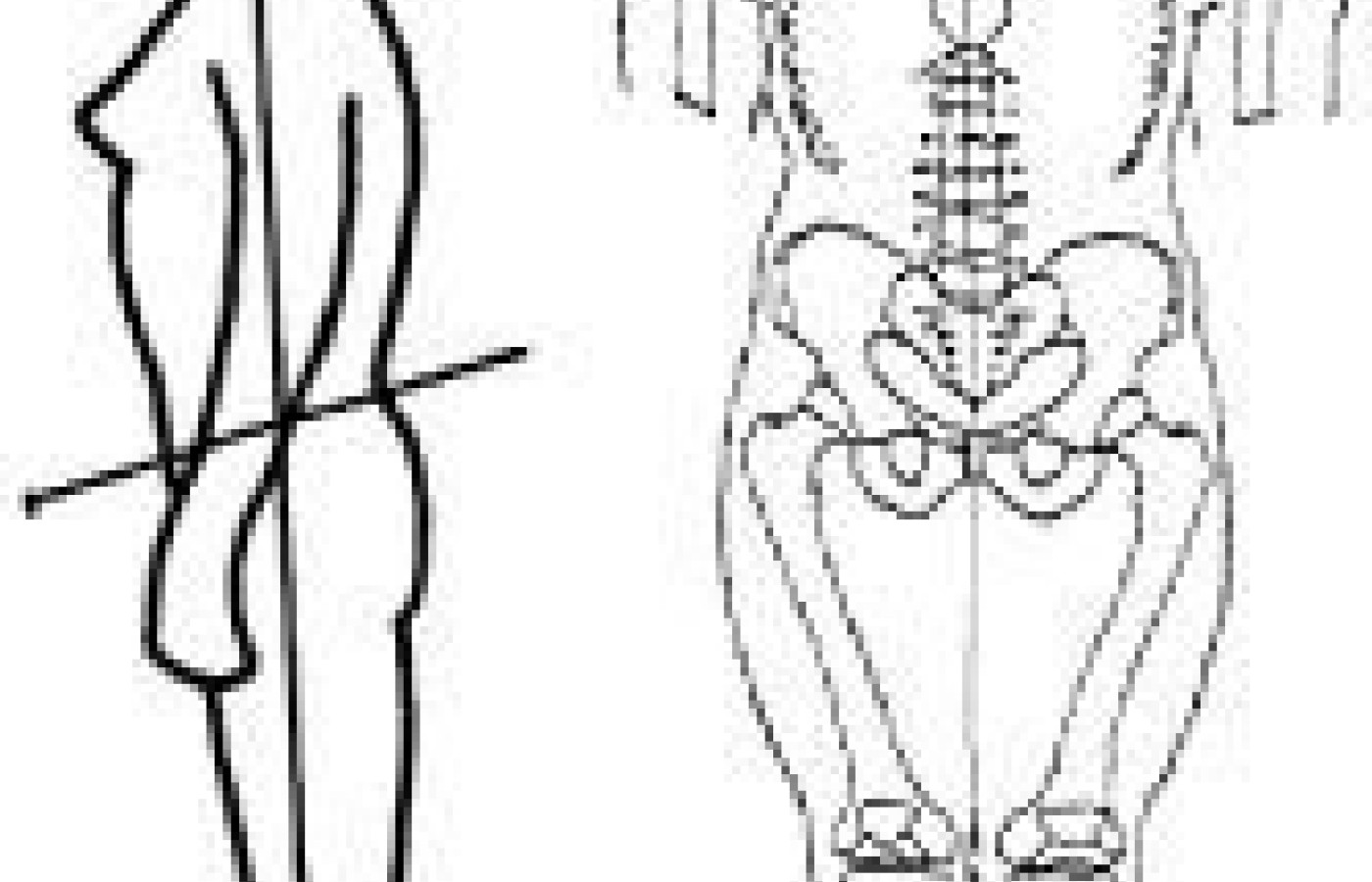
To be able to recognize the attributes of bad posture, one must first have some standard of what constitutes good or normal posture. Fortunately, many authors have discussed the importance of normal posture.1,4,5,7,8Figure I demonstrates normal erect human posture under the conditions of static equilibrium. In the lateral view, normal postural alignment is defined as balance about a coronal line of reference or gravity line that passes through the external auditory meatus, acromioclavicular joints, greater trochanters and lateral malleoli. In the anteroposterior view, approximate skeletal symmetry allows division of the body into symmetrical halves with bisection of the following points: glabella; frenulum; episternal notch; xiphoid process; symphysis pubis; and a point midway between the medial malleoli of the ankle joints.
Figure I: The normal correct human posture.
Of course, radiographic examination may also be helpful in evaluating a patient's posture since the x-ray passes through the patient's three-dimensional posture and is captured as a two-dimensional artifact on the x-ray film. The focus of this article is introductory and general in nature. The complexities of correlating a patient's 3-D posture with their projected 2-D image is a topic of much importance that will be discussed in a later article. For now, let it suffice to say that deviation away from the general guidelines described here could be considered as alterations away from normal posture, the outcome of which can ultimately lead to the development of pain and dysfunction.
Some of the Physiological Effects of Altered Posture
Bad posture is a lifetime scenario for most people. Take, for example, the situation depicted in Figure II. World-renowned physiatrist Rene Cailliet,MD, has demonstrated that if the head weighs 10 pounds and is aligned with the external auditory meatus directly above the acromioclavicular joint, the effective load on the spinal tissues is 10 pounds. However, if the head is translated anterior, the weight exerted by the head is effectively increased by a factor of 10 with each additional inch of forward translation. That is to say, if the abnormal posture presented demonstrates two inches of forward head posture, the effective weight of the head to the supporting tissues is not 10 pounds, but 20 pounds; three inches of forward head posture results in an effective weight of 30 pounds, and so on. It is known that bone and soft tissue can suffer from such postural abnormality.
Figure II: Abnormal posture can have an adverse effect on spinal tissues.
Research has demonstrated that when loads are altered, bone remodels to accommodate the imposed demands.9 Imagine for a moment the shape of the cervical spine of the woman in Figure II. It is likely that her lower cervical spine would be hypolordotic; a situation that could lead to the development of osteophyte formation. Indeed, it has been shown that subjects with hypolordotic cervical spines have a greater incidence of osteophyte formation10 that is probably due to the imposed demands placed on the hard tissue.
The consequences of bad posture are potentially damaging for the soft tissues as well. Evidence exists that some postural positions can compromise neural tissue by changing blood flow to the spinal cord itself.11 Flexed postures have also been associated with intervertabral disc damage.12 Clinically, we have all observed changes in muscle tension and function in patients who sit for long periods in front of computer screens that have not been set up for maximum postural ergonomics. Sustained abnormal postures cause the muscles to contract isometrically, which leads to hypoxia and tissue damage. Remember that connective tissue also adapts to sustained changes in posture.
It is well-known that tendons, ligaments and discs display time- and history-dependent viscoelastic properties that reflect the complex interaction of collagen and the surrounding ground substances and proteins.13-18 When a significant load is applied to spinal tissues and sustained over time, the tissue experiences creep (deformation) and stress relaxation (a decline in internal stress over a period of time). In other words, connective tissues undergo plastic changes that can become permanent. This is probably why many individuals who exhibit the postural abnormalities of the patient in Figure II cannot be placed into proper postural alignment with either short-term active or passive methods.
Patients with uncorrected abnormal postures are left to potentially suffer a wide variety of unpleasant conditions: neurovascular entrapment syndromes, myofascial pain syndromes, chronic strains, and a wide variety of other nonspecific musculoskeletal pain syndromes.1-5,7,19-20 Brendon Reilly, MD, states: " . . . chronic postural disorders are probably the most common initiating or contributory cause of chronic back pain."5
What Should We Do about Bad Posture?
We should acknowledge that PTs, MDs and DCs all appreciate that poor posture is bad and good posture is, well, good. However, this observation by PTs, MDs and DCs is not really surprising, as parents untrained in spinal function also know that poor posture is detrimental. Moms and grandmothers are known for telling their slouching kids to "stand up straight."
What is our standard chiropractic approach for addressing poor posture? Unfortunately, there isn't one that is universally taught in our chiropractic educational institutions. For the most part, we do what grandmothers do, i.e., admonish patients to "stand up straight." Such awareness training is an important first step, but an inadequate approach by itself.
Can standard diversified adjusting, Activator adjusting, SOT adjusting, or similar adjustments correct longstanding postural imbalances? Unfortunately, there is little evidence to suggest that adjustments of any kind will substantially influence a patient's postural alignment. This leaves the chiropractic profession between the proverbial rock and a hard place. We know posture is an important factor in health, but we have no real effective tools in our standard chiropractic arsenal to address the problem.
In our next column, we will further discuss the attributes of normal upright resting posture and how to assess whether or not the subject under investigation has normal posture, and how to classify their abnormalities of posture. In future columns, we will investigate the works of chiropractic and medical innovators and their specific approaches to postural rehabilitation.
References
Donatelli R, Wooden M. Orthopaedic Physical Therapy. New York: Churchill Livingstone Inc., 1989.
Cailliet R. Low Back Pain Syndrome. Philadelphia: FA Davis Co., 1981.
Cailliet R. Neck and Arm Pain. Philadelphia: FA Davis Co., 1981.
Cailliet R. Soft Tissue Pain and Disability. Philadelphia: FA Davis Co., 1977.
Reilly B. Practical Strategies in Outpatient Medicine. Philadelphia: WB Saunders Co., 1984.
Kendall FP, McCreary EK, Provance PR. Muscles: Testing and Function. 4th ed. Baltimore: Williams & Wilkins, 1993.
Lee D. Principles and practices of muscle energy and functional techniques. In: Grieve GP (ed.) Modern Manual Therapy of the Vertebral Column. New York: Churchill Livingstone, 1986.
White AA, Panjabi MM. Clinical Biomechanics of the Spine. Philadelphia: JB Lippincott Co., 1978.
Rubin CT, Lanyon LE. Osteoregulatory nature of mechanical stimuli: function as a determinant for adaptive remodeling in bone. J Orthop Res 1987;5:300-310.
Gore DR, Sepic SB, Gardner GM. Roentgenographic findings of the cervical spine in asymptomatic people. Spine 1986;6:591-694.
Adams CBT, Logue V. Studies in cervical spondylotic myelopathy part I: movements of the cervical roots, dura, and cord and their relation to the course of the extrathecal roots. Brain 1971;94:557-568.
Woo S, Livesay GA, Runco TJ, Young EP. Structure and function of tendons and ligaments. In: Mow VC, Hayes WC (eds.) Basics Orthopaedic Biomechanics, 2nd ed. Philadelphia: Lippincott-Raven; 1997, p.209-52.
Hukins DWL, Kirbby MC, Sikoryn TA, Aspden RM, Cox AJ. Comparison of structure, mechanical properties, and functions of lumbar spinal ligaments. Spine 1990;15:787-95.
Adams MA, Dolan P. Time-dependent changes in the lumbar spine's resistance to bending. Clin Biomech 1996;11:194-200.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.