One of the challenges we have with shoulder pain is determining if the cause of the pain is an impingement syndrome; the next challenge is to determine if a soft tissue treatment will be beneficial. A soft tissue treatment will be beneficial if the site of impingement is subacromial, rather than intra-articular.
There are a variety of tests for determining impingement: the Neer and Hawkins tests,1 and other indicators from a shoulder examination. But a major question is determining if the impingement pressure is occurring in the subacromial area, that is: a thickened and inflamed subacromial bursa; erosions on the coracoacromial ligament and undersurface of the acromion; and bursal-side partial or full-thickness tearing of the rotator cuff. Or is the impingement pressure more intra-articular: internal posterosuperior glenoid impingement; microinstability causing a secondary impingement; middle glenohumeral ligament tearing; labial tears; anterior glenoid erosions; SLAP (superior labial lesion); chondral lesions; or failure of the humeral head to normally translate posteriorly with maximum external rotation.
There are tests to help determine intra-articular possibilities,2 but a major reason for differentiating subacromial from intra-articular (from a soft-tissue treatment point of view) is that soft tissue treatment is not very effective for intra-articular lesions.
Zaslav3 developed an internal rotation resistance strength test to differentiate between outlet (subacromial) and nonoutlet (intra-articular) causes of shoulder pain in patients with a positive impingement sign. The test was found to have an 88 percent positive predictive value; a 96 percent negative predictive value; an 88 percent sensitivity; a 96 percent specificity; and a 94.5 percent accuracy.
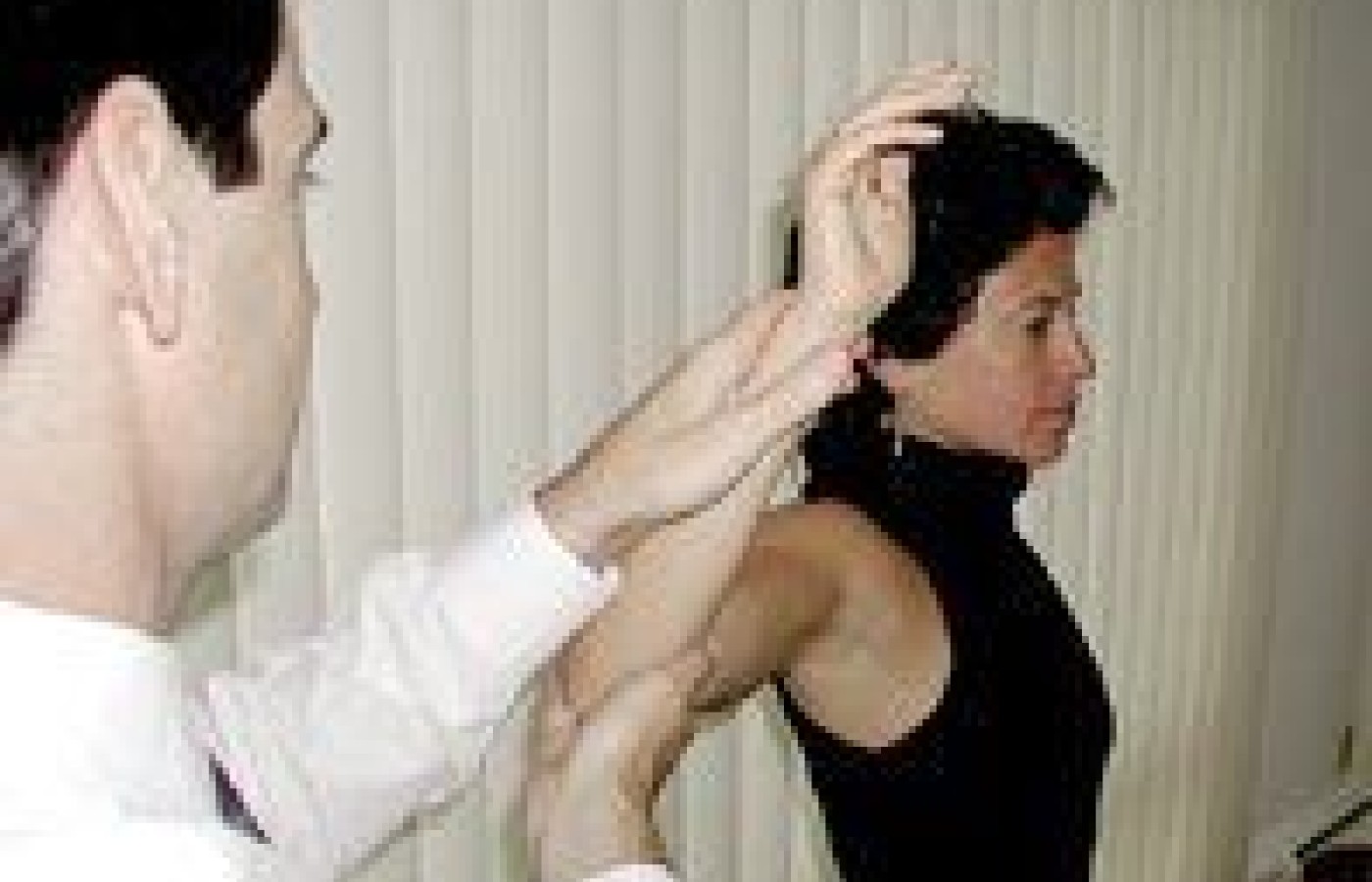
The internal rotation resistance strength test (IRRST) is performed by the examiner standing behind the patient. The patient's arm is in 90° of abduction in the coronal plane, with the forearm in 80û of external rotation (Figure 1). In this position the forearm is isometrically resisted for external rotation, and then compared with internal rotation isometric testing2 (Figure 2). The IRRST is considered positive if, along with a previous positive impingement test, there is good strength in external rotation and apparent weakness in internal rotation. "Because this is a test of relative weakness in a pathologic shoulder, strength is not compared with the opposite side."2 A positive test indicates an intra-articular, nonoutlet impingement, while a negative test (more weakness and probable pain in external rotation) indicates a subacromial outlet impingement.
Figure 1: Resisted external rotation at 80° to 85° in the coronal plane.
Figure 2: Resisted internal rotation at 80° to 85° in the coronal plane.
The biomechanical theory for the positive test of an "apparent" rather than a "true" weakness in internal rotation is as follows: with resistance of internal rotation in the 80° to 85° external rotation position, a vector is created that pushes the humeral head anteriorly toward the anterior glenoid rim and labrum. Tension also occurs along the biceps labial complex and the capsulolabral border "so that pain from both subtle subluxation and biceps and SLAP lesions will be magnified in this position, causing the appearance of weakness."2 This internal resistance position results in a forward movement of the humeral head, thereby reducing the normal obligate posterior translation that occurs with external rotation. This causes the rotator cuff to be contacted between the superior glenoid and humeral head, which produces pain. The authors feel that this test is especially helpful in the more subtle forms of internal and secondary impingement related to instability in the younger patient. In the 50-year and older population, there was more weakness in external rotation (94 percent); the younger-than-50 population exhibited more weakness in internal rotation (66 percent of the time.) This test agrees with present-day research indicating that younger patients suffer with more instability than older patients in the shoulder area.
I have found this test to be very useful in differentiating the location of the impingement lesion.
Hammer WI. Functional Soft Tissue Examination & Treatment by Manual Methods: New Perspectives, 2nd edition. Gaithersburg, MD, Aspen, 1999.
Zaslav KR. Internal rotation resistance strength test: A new diagnostic test to differentiate intra-articular pathology from outlet (Neer) mpingement syndrome in the shoulder. J Shoulder Elbow Surg, Jan/Feb 2001.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.