The separated shoulder, otherwise known as acromioclavicular (AC) dislocation, is a relatively common injury representing approximately 10 percent of all shoulder dislocations.1 It most frequently involves patients between the ages of 15 and 40, and is commonly seen in athletes.1,2 Rarely will this joint dislocate in children; those who have the clinical appearance of an AC separation tend to have a displaced fracture of the distal clavicle instead.1
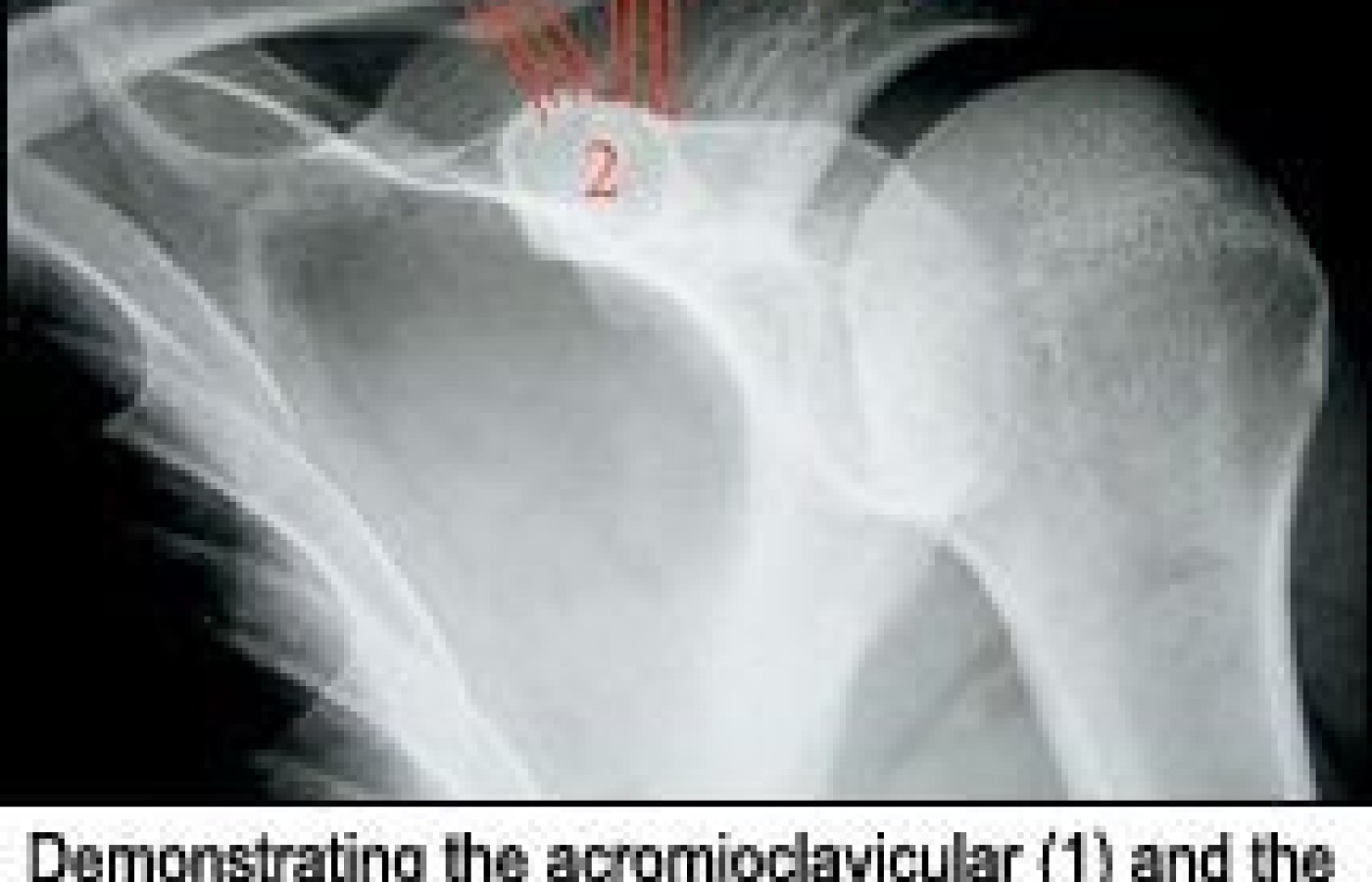
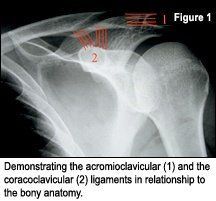
Several mechanisms of injury will induce a separated AC joint, including a downward blow to the lateral shoulder (forcing the acromion downward), a fall on the outstretched hand (forcing the clavicle upward) and tractioning the arm away from the chest wall.1,2 No matter the mechanism of injury, the damage to the acromioclavicular and coracoclavicular ligaments (Figure 1) varies depending upon the applied force. The resulting injury ranges between mild, moderate and severe sprain.1-4 Patient symptoms will vary according to the degree of injury and range anywhere from mild tenderness and swelling with limited range of motion to a complete inability to abduct the arm.2
Radiographic Evaluation
The radiographic evaluation for AC separation stems around the relationship of the clavicle to the acromion and coracoid processes. The region should be evaluated in both the neutral and weight-bearing (stressed) views bilaterally. The best view to asses this region is an AP projection with a 15-degree upward tube tilt. To properly stress the AC joint, the patient should grasp 5-pound to 10-pound weights and relax the shoulder, trying to avoid stabilizing the area by tensing the shoulder muscles.
There are three regions to evaluate when assessing AC separations radiographically
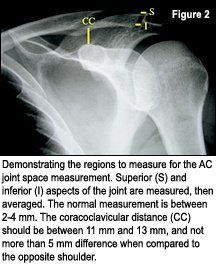
Acromioclavicular distance: This distance is determined by measuring both the superior and inferior aspect of the AC joint (Figure 2) and taking the average. The range should be approximately 2 mm to 4 mm, with no more than 3 mm of difference from right to left sides.1,3
Acromioclavicular alignment: The inferior borders of the distal clavicle and proximal acromion should be in horizontal alignment, with no elevation of the distal clavicle relative to the acromion process.1,3
Coracoclavicular distance: This distance is determined by measuring the most inferior border of the clavicle and the most superior portion of the coracoid process (Figure 2). It should be between 11 mm and 13 mm. There should be no more than 5 mm of difference from the right to left sides.1,3
Classification of Acromioclavicular Injuries
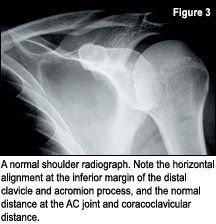
Grade I (mild sprain): In the mild sprain, the acromioclavicular ligament has been stretched with mild tearing, if any at all. The coracoclavicular ligament is not damaged. The AC joint is stable and the position of the clavicle is normal.1,3,4 Radiographically the position of the clavicle remains normal even on weight-bearing (downward traction) radiographs.3 This injury is diagnosed clinically and is radiographically normal (Figure 3).1
Grade II (moderate sprain): In the moderate sprain, the acromioclavicular ligament is torn and the coracoclavicular ligament has been stretched, but is still intact.
Radiographically there is mild elevation of the distal clavicle relative the acromion process, widening of the AC joint or both.1,3,4 Also, there may be calcification seen at the site of the damaged ligaments (posttraumatic heterotopic bone).3 This heterotopic bone is more likely to be present in grade II and grade III injuries, and can be seen in up to 70 percent of cases.1
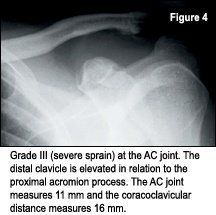
Grade III (severe sprain): In the severe sprain, the acromioclavicular and coracoclavicular ligaments are both torn. Some may have an intact coracoclavicular ligament with an avulsion fracture at the ligament attachment to the coracoid process.1,3,4 On physical inspection, there is a very obvious elevation of the distal clavicle. Radiographically there is widening of the AC joint, obvious elevation of the distal clavicle relative to the acromion process, and widening of the coracoclavicular joint space greater than 13 mm or greater than 5 mm difference when compared to the uninjured side. This injury results in an unstable clavicle (Figure 4).1,3,4
Treatment
In general, conservative management consisting of traditional sprain strain treatment protocol will apply for the grade I (mild sprain). Ice, cross-friction massage and range-of-motion exercise all can be beneficial to the patient. The treating chiropractor may want to refrain from adjusting the AC joint for several weeks, allowing the sprained ligaments to heal before stressing them.
With a grade II (moderate sprain) or grade III (severe sprain), conservative management is beneficial. In addition, both require bracing and either could require surgery to restore stability to the shoulder girdle. There is more and more evidence suggesting that conservative, nonsurgical management is beneficial for a grade III severe sprain at the AC joint.3
Conclusion
The separated shoulder is one of the more common injuries to the shoulder; frequently, patients present themselves to the chiropractic office. This condition can be diagnosed easily through history and radiographic evaluation, as outlined above. The chiropractic setting is very appropriate for the necessary treatment and rehabilitation of this injury. If necessary, an orthopedic referral can be made.
References
Resnick D, Niwayama G. Diagnosis of Bone and Joint Disorders, 3rd edition. Philadelphia: W.B. Saunders, 1995.
Greesnspan A. Orthopedic Radiology: A Practical Approach, 3rd edition. Philadelphia: Lippincott Williams & Wilkins, 2000.
Yochum T, Rowe L. Essentials of Skeletal Radiology, 3rd edition. Baltimore: Williams & Wilkins, 2005.
Marchiori D. Clinical Imaging With Skeletal, Chest and Abdomen. St. Louis: Mosby, 1999.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.