In previous articles in this series, we expounded on the importance of the gluteus maximus (GM) in athletic performance and protecting the knee from injury. We also know there is a link between iliotibial band syndrome and GM weakness. The famous spinal researcher, Stuart McGill, has coined the phrase "gluteal amnesia" to describe GM inhibition. Gluteal amnesia or inhibition may be a result of hip pain.1
McGill found that lower-back-pain patients tend to have gluteal inhibition, which results in dominance of the hamstring muscle for hip extension.2 This hamstring dominance increases the force load on the anterior capsule of the hip and the labrum.3 Weak or inhibited gluteal muscles increase the likelihood of injury and impede athletic performance. Hip or back injury can cause gluteal inhibition, as can the sedentary lifestyles of modern living.
Activating the Gluteus Maximus With Exercise
Most of the exercises we present here are performed weight-bearing in a closed kinetic chain. For some patients with a greater degree of infirmity, we may use exercises like the clam (see description later in article), but we prefer not to isolate muscles from their functional motion patterns.
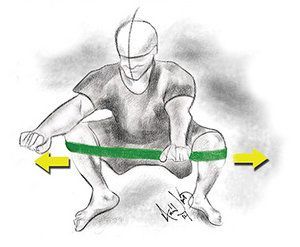
Squat with Exercise Band
1. Squatting
We all squat hundreds of times per day; every time we raise from a chair, car seat or commode, we are performing a squat. One of the factors that restricts geriatric patients from independent living is the inability to rise from a seated position. While our patients may progress to weighted squats, we need to ensure that they develop good form with body-weight squats prior to adding resistance.
Technique:
Stand with feet wider than shoulder-width apart and toes pointed outward. This has been called an athletic stance. The feet should grip the ground with an external rotation force (although they should not move).
Stiffen the core muscles by bracing your abdominals, neither pulling them in nor pushing them out.
While maintaining a lumbar lordosis, descend with the buttocks moving down and backward. The motion should occur through the hip in a hip hinge. The shins should remain perpendicular or nearly perpendicular to the floor.
Descend until the femurs are parallel to the floor or until you can no longer maintain your lumbar lordosis. (Not everyone will be able to perform deep squats.)
The torso can move forward as long as the lumbar lordosis is intact. The arms may be extended forward to act as a balancing cantilever while performing body-weight squats.
Monster Walks
Progression:
Once the body-weight squat has been mastered, resistance may be added. Instead of beginning with a barbell, begin with the resistance of exercise tubing. Place the tubing at or above the knee and perform a squat while maintaining pressure against the resistance of the band. Once this is mastered, weighted squats with exercise bands may be added.
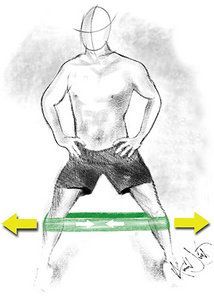
2. Monster or Sumo Walks
Place an exercise band around the knees, ankles or forefoot.4 Next, separate the legs until the band is taut and the legs are at least 14 inches apart. While maintaining constant tension on the band, descend into a quarter-squat. Walk forward to perform monster walks or sideways to perform sumo walks. Do not let the exercise band lose tension while performing either exercise.
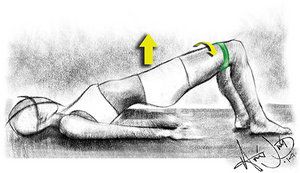
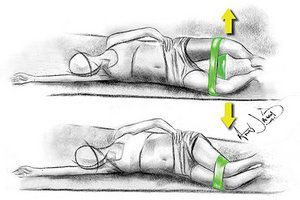
Hip Thrusters with Exercise Band
3. Hip Thrusters With Exercise Bands
This exercise is performed from the supine position with the legs bent. Place an elastic exercise band just above or below the knees. Spread the thighs until tension is felt and the GM is engaged; then rise up to a bridged position. A weighted bar may be placed across the pelvis to increase resistance.
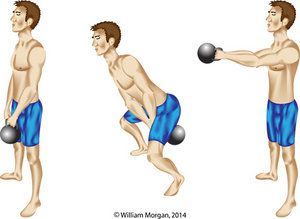
4. Kettlebell Swings
Kettlebell swings are a great dynamic exercise for activating the gluteal muscles, but may be difficult to master without personal coaching. Grip the kettlebell with two hands, palms down. The lumbar arch should be maintained, with the chest out and shoulders back, the core stiffened, and the head facing forward.
Kettlebell Swings
Begin by spreading the legs (standing in an athletic stance) with the toes pointing outward approximately 30 degrees. This is not a squatting motion (do not bend to 90 degrees) or a shoulder isolation exercise; it is a hip-hinging exercise.
Begin by sitting back. The kettlebell swings back between the legs as it reaches end range and the hips "pop," propelling the kettlebell forward. Remember, this is not a shoulder exercise. Use the momentum of the hip motion to propel the kettlebell forward.
Do not attempt to lift or pull the kettlebell upward with your arms or shoulders. Practice will be required to get the rhythm of this athletic motion pattern. This is a relatively advanced exercise.
5. Lunges
Lunges should be performed with the same principles used for squatting. Maintain the lumbar lordosis, keep the tibia parallel to the ground, and stiffen the core.
While watching yourself in the mirror, step forward with one leg. Keep upright with your shoulders back and your chest out. Descend until your femur is parallel to the ground. Your front foot should remain flat on the ground, while the posterior foot may bend so that only the ball of the foot is in contact with the ground.
Make sure your knee remains in alignment with the hip and shin. Do not allow the knee to migrate medially. Return to standing, upright position and repeat on the other side.
Clams
6. Clams
Clams are not our preferred gluteal exercise due to their isolation of the external rotators of the hip. However, there are patients who are unable to perform the compound exercises we have previously proposed. In such cases, clams are performed with a resistance band placed just above the knees with the patient in side-lying position. The knees are bent and feet are together. The patient then opens the knees like a clam opening its shell to approximately 50 degrees. Perform repetitions on each side.
This portion of our series introduces the clinician to various ways to activate the gluteal muscles. It is incumbent upon the clinician to implement a program of gluteal invigoration. Some patients will be able to start with more advanced exercises like weighted band squats or kettlebell swings; while others will never be able to perform these exercises and may need to start with clam exercises.
We recommend you teach most patients the basics of squatting and begin with monster or sumo walks to activate the GM. We also recommend you highlight the lifestyle components of gluteal inhibition, such as excessive sitting and inactivity.
Editor's note: This article is the latest in an ongoing series by Drs. Morgan and Javid on chiropractic management of lower extremity conditions.
References
Freeman S, Mascia A, McGill S. Arthrogenic neuromusculature inhibition: a foundational investigation of existence in the hip joint. Clin Biomech, 2013 Feb;28(2):171-7.
McGill S. Low Back Disorders: Evidence-Based Prevention and Rehabilitation, Second Edition. Champaign, IL. Human Kinetics: 2007.
Lewis CL, Sahrmann SA, Moran DW, Anterior hip joint force increases with hip extension, decreased gluteal force, or decreased iliopsoas force. J Biomech, 2007;40(16):3725-3731.
Cambridge ED, Sidorkewicz N, Ikeda DM, McGill SM. Progressive hip rehabilitation: the effects of resistance band placement on gluteal activation during two common exercises. Clin Biomech, 2012 Aug;27(7):719-24.
Additional Resources
Farrar RE, Mayhew JL, Koch A. Oxygen cost of kettlebell swings. J Strength Conditioning Res, 2010 Apr;24(4):1034-6.
Jay K, Frisch D, Hansen K, et al. Kettlebell training for musculoskeletal and cardiovascular health: a randomized controlled trial. Scand J Work, Environ & Health, 2011 May;37(3):196-203.
Brumit J, Gilpin H, Brunette M, et al. Incorporating kettlebells into a lower extremity sports rehabilitation program. North Amer J Sports Phys Ther, 2010 December;5(4):257–265.
When sports chiropractors first appeared at the Olympic Games in the 1980s, it was alongside individual athletes who had experienced the benefits of chiropractic care in their training and recovery processes at home. Fast forward to Paris 2024, where chiropractic care was available in the polyclinic for all athletes, and the attitude has now evolved to recognize that “every athlete deserves access to sports chiropractic."
It is estimated that 61% of patients with CTS avoid taking surgical options due to postoperative complications and costly surgical procedures. Chiropractic care offers a comprehensive and effective treatment for carpal tunnel syndrome, addressing the condition from multiple angles. Recent studies also have unveiled a game-changing adjunct to chiropractic treatments for CTS: nerve flossing.
Some doctors thrive in a personality-based clinic and have a loyal following no matter what services or equipment they offer, but for most chiropractic offices who are trying to grow and expand, new equipment purchases help us stay relevant and continue to service our client base in the best, most up-to-date manner possible. So, regarding equipment purchasing: should you lease, get a bank loan, or pay cash?